Role of Parental Overprotection and Stressful Life Events in Occurrence of Anxiety Disorders
Sadaf Mansab and Humaira Mohsin (Ph. D.) Centre for Clinical Psychology,
University of the Punjab
The present study aimed to investigate the role of perceived parental overprotection during childhood and experiences of stressful life events, as possible risk factors for the development of anxiety disorder in adulthood. Retrospective Ex post Facto Design was used as research design. The sample consisted of 400 adults (age range = 18 - 53 years); divided into clinical group (n= 200) and control group (n = 200). Symptom Checklist-R Anxiety subscale (SCL-A), Parental Bonding Instrument (PBI) and Social Readjustment Rating Scale (SRRS) were administered. Independent sample t-test and Regression analysis were applied to analyze the data. The results showed that clinical group perceived their fathers and mothers significantly more overprotective and less caring than control group. Clinical group scored significantly higher on the Social Readjustment Rating Scale as compared to control group. Regression analysis revealed that mother overprotection positively predicted and father care negatively predicted anxiety in clinical group.
Keywords: overprotective parenting, stressful events, anxiety disorders.
There is diverse spectrum of anxiety problems that exist in every culture ranging from nervousness, avoidance, shyness to full criterion followed Anxiety Disorders. Overall prevalence of Anxiety Disorders in Pakistan is found to be 34% (Mirza & Jenkins, 2004). Anxiety Disorders were reported to be the second most prevalent psychological disorders among adults of Lahore City. The prevalence of Anxiety Disorders was accounted to be 1.12% in adult males and remarkably high in adult females i.e 4.01 % (Rehman et al., 2008). Due to high prevalence rate, it seems important to study the factors that lead to the development of Anxiety Disorders in Pakistani society.
Keeping aside the genetic factors for any psychopathology, many studies in the past focused on the environmental aspects such as overprotective and strict parenting, family maladjustments, lack of socialization, financial problems and stressful life events, that were linked to psychological problems, particularly Anxiety Disorders (Anna, Muris, Susan, & Thomassen, 2006; Berg-Nielsen, Vikan & Dahl, 2002: Carter, Sbrocco, Lewis, & Friedman, 2001; Edwards, Rapee, & Kennedy, 2009; Fox, Halpern, Ryan, & Lowe, 2010; Gilbert, Allan, & Goss, 1996; Girolamo, Dietrich, & Angermeyer, 2008; Gothelf, Aharonovsky, Horesh, Carty, & Apter, 2004; Heider et al., 2009; Manfro et al., 1996; McLaren & Crowe, 2003; McLaughlin & Hatzenbuehler, 2009; McLeod, Wood & Weisz, 2007; Middeldorp, Cath, Beem,Willemsen, & Boomsma, 2008; Mofrad, Abdullah, & Samah, 2009; Muris et al., 2006; Ollendick, Langley, Jones, & Kephart, 2001; Sideridis & Kafetsios, 2008; Someya et al., 2000; Spokas & Heimberg, 2009; Takahashi, 2000; Taylor & Alden, 2006; Thomasgard & Metz, 1993; Wilcox et al., 2008; Wilde & Rapee, 2008; Yoshida, Taga, Matsumoto, & Fukui, 2005; Zlomke & Young, 2009).
Therefore overprotective parenting and stressful life events were chosen for the present research to find out their involvement in the development and maintenance of Anxiety Disorders in adult life.
Overprotective parenting, one of the main constructs of the present study, has been researched widely in the past. Levy (1970) defined overprotective relationship characterized by a parent who is highly supervising and vigilant, has difficulties with separation from the child, discourages independent behavior and is highly controlling (as cited in Thomasgard & Metz, 1993). Parker, Tupling, and Brown (1979) formulated overprotection as parental behaviors that disallow the child's personal growth, development, autonomy, and independence. They included a second variable in their model; i.e. care, which depicts the parents' ability to communicate, emotional expression, and promote closeness with the child (as cited in Mofrad, Abdullah, & Samah, 2009). Parker, Tupling, and Brown (1979) also categorized parents according to whether they are high or low on parental overprotection and care.
Child rearing practices are different and diverse in different ethnicities. In South Africa, white youths generally rated their parents' rearing behaviors as less anxious, overprotective, and rejecting, but more emotionally warm than colored and black youths (Muris et al., 2006). In Japanese community, patients with Panic Disorder scored their parents as more rejecting and overprotective than did control group (Someya et al., 2000).
In European nations, high maternal overprotection, authoritarianism and low paternal care was strongly associated with the presence of anxiety disorders such as Panic Disorder With and Without Agoraphobia (PDAG), Generalized Anxiety Disorder (GAD), Social Phobia (SOP) and Simple Phobia (SP) in adults (Heider et al., 2008).
A meta-analysis of studies examined the linkage between parenting and childhood anxiety, it was revealed that parental control and overprotection was more strongly associated with child anxiety than was parental rejection (McLeod, Wood, & Weisz, 2007).
In childhood, perceived parental care, particularly paternal care, was associated negatively with all fears such as fear of failures among students (Sideridis & Kafetsios, 2008). It was found that one of the major risk factor for the development of Separation Anxiety Disorder (SAD) in children is high maternal overprotective parenting style (Mofrad, Abdullah, & Samah, 2009).
In adolescents, insecure attachment and a controlling or anxious rearing style is a strong predictor of anxiety symptoms (Anna, Muris, Susan, & Thomassen, 2006). Similarly, teenage students who recalled maternal overprotection appeared to be at high risk and prospectively predicted an increase in social anxiety in a socially stressful situation such as beginning college life and developing a new relationship etc (Spokas & Heimberg, 2009).
Childhood experiences of parenting have strong impact in adulthood. Those adults who described their parents as overprotective and controlling develop social anxiety and performance anxiety in their adult age (Taylor & Alden, 2006). It was found that adults with a lifetime history of Obsessive Compulsive Disorder were more likely to report parental overprotection and less likely to report parental care, than offspring without such history (Wilcox et al., 2008).
The concept of Stressful Life Events (SLE) given by Holmes and Rahe (1967) has also been linked with physical and mental illnesses extensively. With respect to anxiety disorders, SLE has been an important factor in the occurrence of anxiety disorders in individuals (Barlow & Durand, 2002). Negative and stressful life events were significantly associated with anxiety symptoms and fear, especially when negative life events interact with negative affectivity (Fox & Halpern, Ryan & Lowe, 2010). In causal association of adverse life events and anxiety symptoms; negative attributional style, avoidant coping and emotion dysregulation played the role of mediators (McLaughlin & Hatzenbuehler, 2009; Ollendick, Langley, Jones, & Kephart, 2001).
Children with OCD had experienced significantly more negative life events in the year before onset than normal controls, and they perceived the life events as having more impact (Gothelf, Aharonovsky, Horesh, Carty, & Apter, 2004). It was studied that negative life events, negative attributional style, and avoidant coping, all significantly predicted levels of fear and anxiety (Ollendick, Langley, Jones, & Kephart, 2001).
A research conducted on patients with Panic Disorder, discovered that 79.8% patients reported having had a stressful life event in the year preceding the onset of the disorder (Manfro et al., 1996). Those individuals who had experienced traumatic events of an interpersonal nature had significantly higher levels of PTSD symptoms than those who had experienced other types of events (Lancaster, Melka, & Rodriguez, 2009). Parent anxiety, parent overprotection, child inhibition and the impact of negative life events predicted anxiety in children (Edwards, Rapee, & Kennedy, 2009).
The role of overprotective parenting and stressful life events in the development of Anxiety Disorders has been empirically identified in Western Societies, the present research therefore planned to see the relationship between the variables in Pakistani population.
The present study aimed to explore the role of perceived parental overprotection in childhood and experiences of stressful life events, as possible risk factors for the development of any of anxiety disorders (as listed in DSM-IV TR; Panic Disorder with and without Agoraphobia, Generalized Anxiety Disorder, Obsessive Compulsive Disorder, Social Phobia, Specific Phobia and Post Traumatic Stress disorder) in adulthood.
It was hypothesized that clinical group perceived their parents as overprotective in their childhood and experience more stressful life events as compared to control group. It was also hypothesized that overprotective parenting in childhood and stressful life events were potential predictors of Anxiety Disorders in adult age.
Research Design
Retrospective Ex post Facto Design was used in the present research. The selected participants were already diagnosed with Anxiety Disorders. The present study was also a comparative study, comparing a Clinical Group (participants with anxiety disorders) and Control Group (normal participants). A Purposive sampling (criterion- based sampling) procedure was used to select the required sample.
The research participants were divided into two groups; clinical group and control group. Participants were allotted to clinical and control group on the basis of following criteria
Participant's age should be 18 years and above. He/she should fulfill DSM-IV diagnostic criteria of any Anxiety Disorder (screened by the researcher). He/she must be brought up by at least one biological parent, who was alive till the participant's age was 16 years
Participant's age should be 18 years and above. He/she should have no past and present history of any Anxiety Disorder. He/she must be brought up by at least one biological parent, who was alive till the participant's age was 16 years.
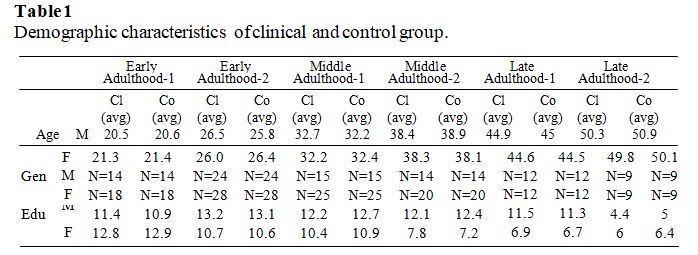
The participants were 400 adults including 176 males (44 %) and 224 females (56%). Both clinical and control groups had equal representation of males (88 + 88) and females (112 + 112). Their age range was 18 - 53 years. In the clinical group, mean age for males was 33.42 years and for females was 32.90 years. In control group, mean age for males was 33.3 years and females mean age was 32.99 years. In clinical group 24 (12 %) adults were illiterate, and 276 (88%) adults were literate, with mean education of 10.46 years. In control group, 14 (7%) adults were illiterate and 286 (93%) were literate with the mean education of 10.43 years.
Both groups were matched on age, gender and education. Each group was divided into six age bands; Early Adulthood-1 (age range 18-23 years), Early Adulthood-2 (age range 24-29 years), Middle Adulthood-1 (age range 30-35 years), Middle Adulthood-2 (age range 36-41 years), Late Adulthood-1 (age range 42-47 years) and Late Adulthood-2 (age range 48-53 years), for precise comparison between the two groups. Age was matched; mean age of each age band in both clinical and control group was approximately same (see Table 1). For gender variable, each group had equal number of male and female participants falling in each age band. Education was also matched; mean education of each age band in both clinical and control group was about the same (see Table 1).
Demographic Questionnaire (in Urdu Language) was constructed by the researcher, that consisted of items which recorded the name, age, gender, religion, education, marital status, occupation, monthly income, parental history of psychological illness, and duration of illness of participants.
Anxiety Disorder Checklist (Rehman et al., 2008): It is an indigenous tool developed for Pakistani population based on DSM-IV TR criteria. It was used to screen out and diagnose the presence of Anxiety Disorders. It had two portions; screening portion and diagnostic portion. Screening portion had 7 questions, for each anxiety disorder (Panic Disorder without Agoraphobia, Panic Disorder with Agoraphobia, Specific Phobia, Social Phobia, Obsessive Compulsive Disorder, Posttraumatic Stress Disorder and Generalized Anxiety Disorder). Diagnostic portion was based on DSM-IV TR criteria for anxiety disorders. All items are scored on “yes” and “no” (score 1 and 0 respectively).
Symptom Checklist-R (Anxiety Scale) (SCL-R; Rehman, Dawood, Rehman, Mansoor, & Ali, 2009): It is an indigenous tool and was used in present study to quantify the anxiety symptoms in research participants. SCL-R responses are rated on a 4-point Likert Scale ranging from 0-3. In the present study, only Anxiety subtest was used. Validity of SCL-A with State Trait Anxiety Inventory (STAI) was reported r = 0.47, p <
0.05. The test-retest reliability of Symptom Checklist Anxiety Scale (SCL-A) for normal population was 0.81 and for psychiatric population was 0.95 (Rehman, Jagin, Dawood, Mansoor, & Rehman, 2009).
Parental Bonding Instrument (PBI; Parker, Tupling, & Brown, 1979): It was used to measure Perceived Parental Care (12 items) and Overprotection (13 items). Items are rated on a 4-point Likert-type scale ranging from ''very like'' to ''very unlike''. Adequate test–retest reliability has also been demonstrated in an undergraduate sample,
i.e. r = 0.86 for Care, r = 0.85 for Overprotection, by Whisman and Kwon (1992). For a clinical sample, test-retest reliability was r = 0.87 for Care, r = 0.92 for Overprotection, discovered by Parker in 1981(as cited in Spokas & Heimberg, 2009). It had adequate Validity, i.e. about 0.77 with semi-structured interview of a non-clinical group assessed the extent to which members described their parents as caring or overprotective and 0.43 to 0.63 with Social Support Questionnaire (SSQ) (as cited in Spokas & Heimberg, 2009). The tool was translated into Urdu for present study by following the standard translation procedure.
Social Readjustment Rating Scale (SRRS; Holmes & Rahe, 1967): It was used to measure how much stress has been faced by participants due to stressful life events in past years. It has good psychometric properties. Reliability for normal individuals ranged from 0·96 to 0·89 and for patients ranged from 0·91 to 0·70 (as cited in Dohrenwend, 2006). For the present research, Adult Form was translated into Urdu by following the standard translation procedure.
The research was carried out at four main research sites of Lahore city; teaching hospitals, Departments of Punjab University, Community and markets places.
In order to assess the comprehension level of translated questionnaires and analyze the possible difficulties in research, a pilot study was conducted on 20 adults (10 from clinical group and 10 from control group). Feedback showed that the comprehension level of all questionnaires was adequate, no fatigue and boredom was reported. Administration of all questionnaires (Demographic Questionnaire, Anxiety Disorders Checklist, SCL-A, PBI and SRRS) took approximately 20-25 minutes.
Initially data from clinical group was taken. Individual administrations were done. Written informed consent was taken from each participant. Once the data was collected from clinical group, control group data was gathered from university students, community and markets places. In community and markets, verbal and written informed consent was taken from each participant. During data collection from Punjab University departments, it was observed that some of the participants fulfilled the diagnostic criteria of some of the anxiety disorders, and it was validated by Anxiety Disorders Checklist. That portion of data (16 adults) was later on included in clinical group because they met the criteria required for clinical group. The data collection process was completed in two months.
Statistical Program for Social Sciences (SPSS- 14 version) was used for statistical analysis. Frequencies, means, standard deviations, independent sample t-tests, step wise regression analysis was computed.
Demographics
The sample was divided into two groups. Both clinical and control groups were matched on age, gender and education. Majority of the participants were Muslims in both groups. In clinical group 24 (12 %) adults were illiterate and 276 (88%) adults were literate, with mean education of 10.46 years. In control group, 14 (7%) adults were illiterate and 286 (93%) were literate with the mean education of 10.43 years. Majority of participants were Muslim in both groups; about 98.5 % in clinical group and 98% in control group. In clinical group, about 77 (38.5%) participants were unmarried, 105 (52.5%) individuals were married, 12 (6%) adults were widow and 6 (3%) females were divorced. Alternatively, in control group, 64 (32%) individuals were unmarried. 129 (64.5%) participants were married, 6 (3%) adults were widowed and 1 (0.5%) females were divorce.
Independent sample t-test for difference between Clinical and Control Group on Father and Mother Care, Father and Mother, Overprotection and Stressful Life Events.
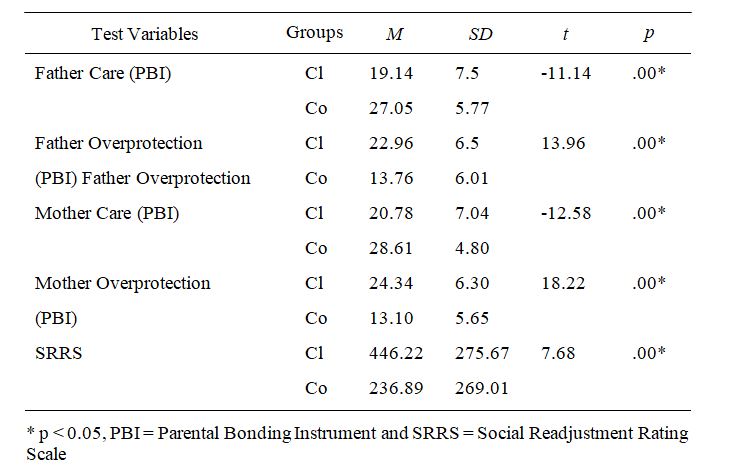
Table 2 showed that the participants of clinical group perceived their fathers and mothers significantly more overprotective than the participants of control group. It also revealed that the participants of clinical group perceived their fathers and mothers significantly less caring than the participants of control group. For Stressful Life Events, the participants of clinical group scored significantly higher on the Social Readjustment Rating Scale as compared to the participants of control group.
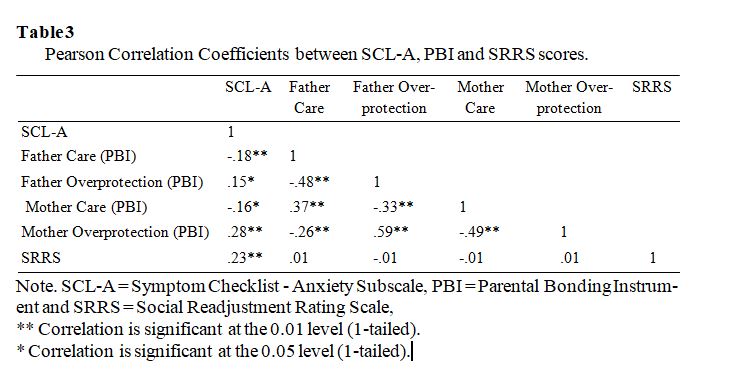
Pearson Product Moment Correlation Analysis was carried out on clinical group to discover any positive or negative correlation between test variables. Table 3 revealed that anxiety scores negatively correlated with father care and mother care. Whereas positive correlation was found with father overprotection and mother overprotection. Similarly, for stress and anxiety also positively correlated
Predictors for Anxiety Level
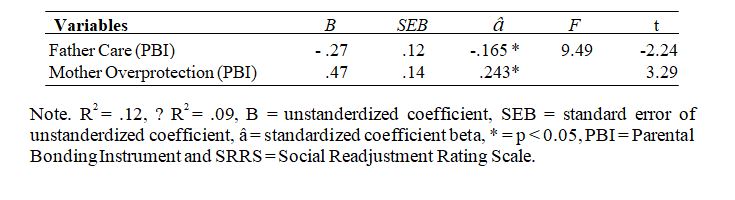
Backward Linear Regression Analysis was carried out on clinical group, to evaluate that the parental overprotection and stressful life events as risk factor for anxiety level in adulthood (Table 4). Regression analysis carried out on clinical group showed that only two out of five test variables, predict anxiety in adult age. Mother overprotection positively predicted while father care negatively predicted anxiety in adult age. Between these two variables, mother's high overprotection is better predictor of anxiety than father's low care. Whereas R2 value was not very strong (R2 = .12); it depicted that only 12% of variance in anxiety level was due to high maternal overprotection and low paternal care.
Regression analysis also revealed that SLEs did not predict maintenance of anxiety symptoms in adulthood in the clinical group.
Regression Analyses with parental care, parental overprotection and stressful life events as predictor of anxiety level.
In the present study, it was hypothesized that the participants of clinical group would perceive their mothers significantly more overprotective than the participants of control group. The present hypothesis was verified statistically. Previously conducted studies also support the result of the present research (Taylor & Alden, 2006; Wilde & Rapee, 2008). So it seems that people in Pakistan also succumb to anxiety disorders as a result of maternal overprotection, like the people in western cultures.
The current findings revealed that adults in clinical group perceived their fathers as more overprotective than the participants of control group. These findings are similar to previous researches. Someya et al. (2000) which demonstrated that Japanese patients with panic disorder perceived their parents, particularly fathers as more rejecting and overprotective than did control subjects. In Pakistani culture, fathers are expected to be strict and authoritarian. Thus the present research also points out that due to excessive control and overprotection from parents, especially from fathers in childhood may produce anxious adults as compared to those who had healthy relations with father.
Existing findings showed that adults in clinical group perceived their mothers as less caring than the participants of control group. The present results confirmed the results of earlier finding, e.g. Someya et al. (2000) established that Japanese patients with agoraphobia reported significantly less emotional warmth and care from mothers in their childhood. Additionally, Heider et al. (2008) found that maternal care showed significant inverse associations with the occurrence of Panic Disorder With and Without Agoraphobia (PDAG), Generalized Anxiety Disorder (GAD), Social Phobia (SOP) and Specific Phobia (SP). In Pakistan, the controlling behavior of mothers' perhaps imbalances the amount of care they should give to their children. This inapt parenting probably makes the child confused about its internal strengths in crucial situations and hence increases his anxiety which is reflected through behavioral manifestation.
Another conclusion of present study was that the participants of clinical group would perceive their father significantly less caring than the participants of control group. The given assumption was earlier supported by Heider et al. (2008). Children usually consider their fathers the symbol of strength and protection. This idealization makes their fathers as a role model for them, who support them in time of danger and helped them to learn how to encounter threats in everyday life. But in Pakistani culture, the controlling and overprotective behaviors of fathers, uneven the quantity of warmth, care and love they should give to their children. Fathers in Pakistan are usually strict and punish their child on his mistakes. As a result, child is unable to take initiative due to the fear of making errors and develops low self-confidence. Such parenting style destroys the decision making power of the child in critical circumstances and distorts their threat perception. Therefore, child may develop anxiety symptoms, which may lead to anxiety disorders in adulthood.
In the present research, it was hypothesized that the participants of clinical group would score significantly higher on the Social Readjustment Rating Scale than the participants of control group. The results confirmed the hypothesis. This notion was validated by Gothelf, Aharonovsky, Horesh, Carty, & Apter (2004) who in their study found that children with OCD had significantly more negative life events in the year before onset than normal controls, and they perceived the life events as having more impact. Similarly, Lancaster, Melka, & Rodriguez (2009) had also demonstrated earlier that those who had experienced a traumatic event reported significantly higher levels of PTSD symptoms than those who had experienced a non-traumatic life event. People in Pakistan have been exposed to a lot of negative life events e.g. bomb blasts, floods, earth quakes etc. along with these traumatic events, there are lots of daily hassles that play role in adjustment difficulties. A study carried out in Lahore discovered that Adjustment Disorder with anxiety features was remarkably more prevalent in adult groups; i.e. 6 % (Rehman et al., 2008). Due to poor coping skills and lack of positive approach, they are remarkably influenced by any stressful incident, which may be further associated to the anxiety symptoms manifestation as compared to those individuals who had never been into such traumatic events or has less experience than those who scored high on SRRS.
Another major concern examined by the present study was whether the high perceived maternal overprotection would be the predictor of anxiety in adulthood. The present study supports the concept of affects of high maternal overprotection as a predictor of anxiety symptoms in adulthood that was given by the previous researches (Heider et al., 2008; Sideridis, & Kafetsios, 2008; Taylor & Alden, 2006).
Correspondingly, the findings of present study were also supported by Mofrad, Abdullah, and Samah (2009) findings, which provided evidences that the high protection by mothers is an antecedent for the experience of Separation Anxiety Disorder symptoms in children. In Pakistani culture, women are not exposed to external environment and have minimal opportunities to make decisions. The limited submissive social role blurred their abilities of risk taking, decisions making, accurate perception of threat and internal locus of control. They are afraid to change and usually have low frustration tolerance. When they become mothers, these characteristics build a parenting style, which is very controlling because mothers believed that if the child gets out of their control, he may be in danger. This parenting style discourages child's independence, risk taking, actual threat perception and decision making. The child brought up in such environment reflects the characteristics; i.e. get easily nervous, consistently worries about his social image, fear failure (Social Phobia), develop irrational fear of neutral objects and situations (Specific Phobia), catastrophizes the bodily symptoms and external threats (Panic Disorder), shows excessive worry about cleanliness, insecurity manifested in compulsive checking, perfectionism (OCD), avoids stressful situations and recollections (PTSD), experiences free floating anxiety and worries about being worried (GAD).
It was expected that high perceived paternal overprotection would be the predictor of anxiety in adulthood. The hypothesis was rejected. The research conducted by Carter, Sbrocco, Lewis, and Friedman (2001) also supports this finding. They concluded that African Americans verified a similar negative relationship between anxiety and care, but no relationship was evidenced between anxiety and paternal overprotection. Similarly, another study conducted by Wilcox et al. (2008) reported that there is no significant association between paternal overprotection and offspring's OCD. It was generally observed that in our Pakistani culture, father's role has not been warm and welcoming for the children and current research discovered that fathers in our society were overprotective. But their overprotection didn't contribute to development of anxiety disorders in adulthood. This might be because paternal overprotection was characterized by behavioral control, i.e. not giving permissions to child to stay out for long hours, not allowing child to make his own decisions and compelling child to follow discipline etc. Father overprotection is not been illustrated by psychological control, i.e. considering that the child can't take care of his self until parents are around, unlike child's independence, considering child as kid even he/she has grown up, maintaining a close proximity with child etc. Due to behavioral control, paternal overprotection might be considered as part of child training rather than anxious and overprotective parenting.
Another hypothesis of existing study was that low perceived maternal care would be the predictor of anxiety in adulthood. The hypothesis was also rejected. From a cultural perspective, one reason for such findings might be, that when proper care and warmth was not given by the mother to the children, they found other attachment figures nearby, i.e. father, grandparents (both maternal and paternal), maternal or paternal aunts or uncles (Mamoo, Khala, Phuphu or Chacha) or any elder sibling for secure attachment and emotional needs. In these circumstances, children have minimal chances of developing any anxiety disorder because lack of maternal care was compensated by any other caregiver. Similar findings were revealed by Hodges and Tizard (1989), they negated the Bowlby Attachment Theory on monotropy, i.e. institutionalized children were not significantly different from non-institutionalized children in personality development, though some qualitative differences were identified. This shows that lack of care given by mother does not play any role in the development of Anxiety Disorders, because the child can find any other attachment figure and develop somehow normally.
Furthermore, an important issue focused in the current study was that the low perceived paternal care would be the predictor of anxiety in adulthood. This supposition was found to be true. Previous literature also supports this postulation (Heider et al., 2008; Sideridis & Kafetsios, 2008). In Pakistani society, the controlling and overprotective behavior of fathers overweight the quantity of warmth, care and love they should give to their children. This inconsistent parenting style can have onus on the decision power of child in critical circumstances; and therefore child may develop anxiety symptoms, which may lead to anxiety disorders in adulthood.
Finally, it was hypothesized that Stressful Life Events would be the predictor of anxiety in adulthood. This assumption was rejected. This result of the present study was not supported by previous literature (McLaughlin & Hatzenbuehler, 2009; Ollendick, Langley, Jones, & Kephart, 2001). The present research findings did not match with the previous studies because all researches had some additional variables (neuroticism, extraversion, negative attributional styles, avoidant coping and emotional dysregulation etc). The association of stressful life events and anxiety symptoms may have been intervened by these variables. These additional variables might be having mediating, moderating or interacting effects on anxiety symptoms with respect to stressful life events. Secondly, SRRS was only translated for the current study and not adapted according to Pakistani culture. In our society, death of spouse was not that much stressful (Score 100 on SRRS) as compared to change in financial conditions and trouble with in- laws (Score 38 and 29 respectively). Due to this, although participants scored very high on SRRS quantitatively, but qualitatively they are not that stressed to have a chance of developing and maintaining any illness (physiological and psychological).
In conclusion, the present study found that people with anxiety disorders perceived their parents more overprotective and less caring as compared to those who had not diagnosed with any anxiety disorder. Moreover, parental overprotection and experience of stressful life events positively correlated with anxiety level, whereas, parental care negatively correlated with anxiety level in adults. The major findings of current research were that the maternal overprotection and paternal low care played a significant role in the development of anxiety symptoms in adulthood.
Parental overprotection was assessed through retrospective reports, and can be biased because childhood memories can fad over time. That is why longitudinal studies are necessary for causal relationship.
Other factors such as parental education, parental illness, individual's personality characteristics, individual's education and social background etc, which might act as mediators or moderators were not taken into consideration. It is suggested to develop theoretical models through qualitative research for in-depth analysis.
In present study, only age, education and gender were matched for comparative groups. It is recommended that for Retrospective Ex post-Facto Design, more variables should be matched for increased validity of results, e.g. socioeconomic status, occupation, family history of psychological illness etc.
The clinical group consisted of participants with Anxiety Disorders and co- morbidities were not ruled out, which might distort the research results. It is recommended that patients suffering with Anxiety Disorders and no comorbid disorder can be selected in the future research to find out the association of parental overprotection and anxiety symptoms.
Majority of participants with anxiety disorders were taken from hospitals and all those who lived in general population were not part of sample. Therefore, it lacks the representation of population (all people with anxiety disorders). It is advised to take sample from both hospitals and community for adequate representation.
Due to limited resources and permissions issues, all hospitals of Lahore city were not represented in the sample. It is proposed that sample should be taken from both government and private hospitals, so that the data represents all socioeconomic classes.
American Psychiatric Association. (2000). Diagnostic and statistical manual of Mental Disorders. (4th ed.) –DSM-IV TR. Washington, DC: American Psychiatric Association.
Anna, M. L., Muris, P., Susan M. B., & Thomassen, C. (2006). A multifactorial model for the etiology of anxiety in non-clinical adolescents: main and interactive effects of behavioral inhibition, attachment and parental rearing. Journal of Child Family Studies, 15, 569-579. Retrieved from http://www.springerlink.com
Barcelona. (2008). Good parent-children relationships can prevent future anxiety disorders. I magazine 'Social Psychiatry and Psychiatric Epidemiology', (N.A). R e t r i e v e d f r o m h t t p : / / w w w. i m i m . e s / m e d i a / u p l o a d / p d f / / P B I %20ansiedad%20ESP%20DEF-EN%20_2 editora_181_12.pdf
Barlow, D. H., & Durand, V. M. (2002). Abnormal psychology: An integrative approach (3rd ed.).United States: Wadsworth Thomason Learning.
Bee, H. (1997). The developing child (8th ed.). New York: Addison-Wesley Educational Publishers, Inc.
Berg-Nielsen, T. S., Vikan, A., & Dahl, A. A. (2002). Parenting related to child and parental psychopathology: a descriptive review. Clinical Child Psychology and Psychiatry, 7, 529-552. Retrieved from http://ccp.sagepub.com/ cgi/ reprint/7/4/529
Carter, M. M., Sbrocco, T., Lewis, E. L., & Friedman, E. K. (2001). Parental bonding and anxiety: Differences between African American and European American college students. Anxiety Disorders, 15, 555-569. Retrieved from http://www.sciencedirect.com.
Rahman et al. (2008). Prevalence of psychological disorders in Lahore city. (Unpublished Bachelors thesis). Centre for Clinical Psychology, University of the Punjab, Lahore.
Comer, R. J. (2006). Abnormal psychology (6th ed.). New York: W. H Freeman & Company.
Darling, N. (1999). Parenting style and its correlates. Retrieved from http://www.athealth.com/Practitioner/ceduc/parentingstyles.html.
Davison, G. C., & Neale, J. M. (2001). Abnormal psychology (8th ed.). New York: John Wiley & Sons, Inc.
Dohrenwend, B. P. (2006). Inventorying Stressful Life Events as Risk Factors for Psychopathology: Toward Resolution of the problem of intracategory variability. Psychol Bull,3,477-495. Retrieved from http://www.ncbi
.nlm.nih.gov/pmc/articles/PMC1584216/
Edwards, S. L., Rapee, R. M., & Kennedy, S. (2009). Prediction of anxiety symptoms in preschool aged children: examination of maternal and paternal perspectives. Journal o f Child Psychology and Psychiatry, ( N A ) . R e t r i e v e d f r o m http://www3.interscience.wiley.com
Fox, J. K., Halpern, L. F., Ryan, J. L., & Lowe, K. A. (2010). Stressful life events and the tripartite model: Relations to anxiety and depression in adolescent females. Journal of Adolescence, 33, 43-54. Retrieved from http://www.science direct.com
Gilbert, P., Allan, S., & Goss, K. (1996). Parental representations, shame, interpersonal problems vulnerability to psychopathology. Clinical Psychology and Psychotherapy, 3, 23-34. Retrieved from http://www3.interscience.wiley.com
Gothelf, D., Aharonovsky, O., Horesh, N., Carty, T., & Apter, A. (2004). Life events and personality factors in children and adolescents with obsessive-compulsive disorder and other anxiety disorders. Comprehensive Psychiatry, 45, 192-198. Retrieved from http://www.sciencedirect.com
Heider, D., Matschinger, H., Bernert, S., Alonso, J., Brugha, T. S., Bruffaerts, R., Girolamo, G. D., Dietrich, S., & Angermeyer, M. C. (2008). Adverse parenting as a risk factor in the occurrence of anxiety disorders. Soc Psychiatry Psychiatr Epidemiol, 43, 266-272. Retrieved from http://www.springerlink.com
Holmes, T., & Rahe, R. (1967). Holmes-Rahe Social Readjustment Rating Scale. Journal of Psychosomatic Research, 11, 213-218. Retrieved from http://www.managingpressure.com/downloads/6_Holmes_and_Rahe_stress_inven tory.pdf
Lancaster, S. L., Melka, S. E., & Rodriguez, B. F. (2009). An examination of the differential effects of the experience of DSM-IV defined traumatic events and life stressors. Journal of Anxiety Disorders, 23, 711-717. Retrieved from http://www.sciencedirect.com
Lazarus, R. S. (1974). Psychological stress and coping in adaptation and illness. International journal of Psychiatry in medicine, 5, 32 I-333. Retrieved from http://www.springerlink.com
Manfro, G. G., Otto, M. W., McArdle, E. T., Worthington III, J. J., Rosenbaum, J. F., & Pollack, M. H. (1996). Relationship of antecedent stressful life events to childhood and family history of anxiety and the course of panic disorder. Journal of Affective Disorders, 41, 135-139. Retrieved from http://www.sciencedirect.com
McLaren, S., & Crowe, S. F. (2003). The contribution of perceived control of stressful life events and thought suppression to the symptoms of obsessive–compulsive disorder in both non-clinical and clinical samples. Anxiety Disorders, 17, 389-403. Retrieved from http://www.sciencedirect.com
McLaughlin, K. A., & Hatzenbuehler, M. L. (2009). Mechanisms linking stressful life events and mental health problems in a prospective, community-based sample of adolescents. Journal of Adolescent Health, 44, 153-160. Retrieved from http://www.sciencedirect.com
McLeod, B. D., Wood, J. J. & Weisz , J. R. (2007). Examining the association between parenting and childhood anxiety: A meta-analysis. Clinical Psychology Review, 27, 155-172. Retrieved from http://www. sciencedirect.com
Mental Health. (2004). Etiology of Anxiety Disorders. Retrieved from http://www.surgeongeneral.gov/library/mentalhealth/chapter4/sec2_1.html
Middeldorp, C. M., Cath, D. C., Beem, A. L., Willemsen, G., & Boomsma D. I. (2008). Life events, anxious depression and personality: a prospective and genetic study. Psychological Medicine, 38, 1557-1565. Retrieved from http://www.tweelingenr egister.org/nederlands/verslaggeving/NTR-publicaties_2008/Middeldorp_ PM_2008.pdf
Mirza, I., & Jenkins, R. (2004). Risk factors, prevalence, and treatment of anxiety and depressive disorders in Pakistan: a systematic review, BMJ, (N.A). Retrieved from http://www.bmj.com
Mofrad, S., Abdullah, R., & Samah, B. A. (2009). Perceived parental overprotection and separation anxiety: Does specific parental rearing serve as specific risk factor. Asian Social Science, 5 ( 11 ) , 109 - 116 . Retrieved f rom h t t p : / / www. ccsenet.org/journal/index.php/ass/article/viewFile/3550/3614
Muris, P., Loxton, H., Neumann, N., Plessis, M. D., King, N., & Ollendick, T. (2006). DSM-defined anxiety disorders symptoms in South African youths: Their assessment and relationship with perceived parental rearing behaviors. Behaviour Research and Therapy, 44,883–896. Retrieved from http://www.sciencedirect.com
Ollendick, T. H., Langley, A. L., Jones, R. T., & Kephart, C. (2001). Fear in children and adolescents: relations with negative life events, attributional style, and avoidant coping. Journal of. Child Psychology, 42, 1029-1034. Retrieved from http://www.psyc.vt.edu
Parker, G., Tupling, H., & Brown, L.B. (1979). A Parental Bonding Instrument. British J o u r n a l o f M e d i c a l P s y c h o l o g y, 5 2 , 1 - 1 0 . R e t r i e v e d f r o m http://www.blackdoginstitute.org.au/docs/ParentalBondingInstrument.pdf
Rajarethinam, R. P., Abelson, J. L, & Himle, J. A. (2000). Acute onset and remission of obsessions and compulsions following medical illnesses and stress. Depression and Anxiety, 12 , 238 - 240 . Retrieved from http:// deepblue. l ib. umich. edu/bitstream/2027.42/35219/1/8_ftp.pdf
Rahman, N. K., Dawood, S., Rehman, N., Mansoor, W., & Ali, S. (2009). Standardization of Symptom Checklist-R on psychiatric and non-psychiatric sample of Lahore city. Pakistan Journal of Clinical Psychology, 8, 21-32
Ray, W. J. (2009). Quasi-Experiments, Correlational and Naturalistic Observational Designs (9th ed), Methods: towards the science of behavior and experiences. USA: Wadsworth Cengage Learning. Inc. Retrieved from http://books.google.com/books
Schwarzer, R., & Schulz, U. (2000). The Role of Stressful Life Events. Retrieved from http://userpage.fu-berlin.de/health/materials/lifeevents.pdf
Sideridis, G. D., & Kafetsios, K. (2008). Perceived parental bonding, fear of failure and stress during class presentations. International Journal of Behavioral Development, 32(2), 119-130. Retrieved from http://jbd.sagepub.com /cgi/reprint /32/2/119
Singh, A. K. (1987). Tests, assessment and research methods in behavioral sciences.
New Dehli: Tata McGraw Hill Publishing Campany.
Someya, T., Kitamura, H., Uehara, T., Sakado, K., Kaiya, H., Tang, S. W., & Takahashi, S. (2000). Panic disorder and perceived parental rearing behavior investigated by the Japanese version of the EMBU scale. Depression and Anxiety, 11,158-162. Retrieved from http://www3.interscience. wiley.com
Spokas, M., & Heimberg, R.G. (2009). Overprotective parenting, social anxiety, and external locus of control: Cross-sectional and longitudinal relationships. Cogn Ther Res, 33, 543–551. Retrieved from http://www.springerlink .com
Taylor, C. T., & Alden, L. E. (2006). Parental overprotection and interpersonal behavior in generalized social phobia. Behavior Therapy, 37, 14-24. Retrieved from http://www.sciencedirect.com
Thomasgard, M., & Metz, W. P. (1993). Parental overprotection revisited. Child Psychiatry and Human Development, 2 4 ( 2 ) . R e t r i e v e d f r o m http://www.springerlink.com
Wilcox, H. C., et al. (2008). The association between parental bonding and obsessive compulsive disorder in offspring at high familial risk. Journal of Affective Disorders , 111 , 31-39. Retrieved from http://www.science direct.com
Wilde, A. D., & Rapee, R. M. (2008). Do controlling maternal behaviors increase state anxiety in children's responses to a social threat? A pilot study. Journal of Behavior Therapy and Experimental Psychiatry, 39, 526-537. Retrieved from http://www.sciencedirect.com
Yoshida, T., Taga, C., Matsumoto, Y., & Fukui, K. (2005). Paternal overprotection in obsessive-compulsive disorder and depression with obsessive traits. Psychiatry and C l i n i c a l N e u r o s c i e n c e s , 5 9 , 5 3 3 - 5 3 8 . R e t r i e v e d f r o m http://www3.interscience.wiley.com
Zlomke, K. R., & Young, J. N. (2009). A retrospective examination of the role of parental anxious rearing behaviors in contributing to intolerance of uncertainty. Journal of Child Family Studies, 18, 670–679. Retrieved from http://www.springerlink.com.