The aim of the present study was to investigate the relationship among coping, self- esteem and quality of life of women with infertility. A sample of 100 women aged above 25 years (M = 30, SD = 4.34) diagnosed with infertility was included. Coping strategies Questionnaire, Rosenberg self-esteem scale - Urdu version and quality of life Brief - Urdu version were used. In the present study Pearson Product Moment Correlation was run for analyzing the relationship between the variables. Coping strategies and quality of life had some significant relationship. A positive correlation was found between Active distracting coping and psychological health related quality of life. A negative correlation was found between Active avoidance coping and psychological health domains of quality of life. Furthermore negative correlation was identified between Avoidance focused coping and psychological health, social relationships and environmental related Quality of life. The results seem to indicate that more the avoidance-focused coping women use the poorer is their quality of life. It can be implied that quality of life of women with infertility needs special attention and healthy coping can help them to better cope with the distress related of infertility.
Keywords: infertility, coping, self-esteem, quality of life
The present study aimed to observe the relationship between coping, self-esteem and quality of life of women with infertility. According to systematic analysis of word wide region in 2010, 48.5 million (45.0 million, 52.6 million) couples were found affected from infertility, the figures are increasing at a faster rate. Furthermore, high prevalence was found in south Asia, Sub Saharan Africa, North Africa/Middle East, and Central/Eastern Europe and Central Asia (Mascarenhas, Flaxman, Boerma, Vanderpoe, & Stevens, 2012). It has been observed that infertility is also the major reproductive problems in Pakistan. In a survey done in Islamabad, in 7628 women 534 were diagnosed with infertility and 7% prevalence was found (Shaheen, Subhan, Sultan, Subhan, & Tahir, 2010).
Infertility primarily refers to the biological inability of a person to conceive after twelve months of unprotected intercourse (Daniluk, 2001). It may also refer to a women's incapability to carry a pregnancy to full term. The time limit of one year is given as normally a couple may need twelve months to achieve conception (Chohan, 2000). Primary infertility is the inability to conceive whereas secondary infertility is the fertility problem after at least one conception (Reid, 2010).
There is a trend in Pakistan that in couples with infertility issues, the blame is automatically placed on the women, even without any investigation of the reasons. Moreover, the label threatens her status in society. The consequences may be severe such as the husband marrying again, giving divorce, or depriving the woman from her inheritance and if these things are not done she may be emotionally, physically or mentally harassed. These consequences are faced in both the cases i.e. primary infertile and secondary infertile women (Parveen, Ahmed, Kausar, Musharaf, Masood, & Afzal, 2008).
Infertility is a source of distress for woman in the society and stigmatizes women with infertility at personal, interpersonal and emotional levels. The women with infertility mostly bear these societal pressures (Fido, 2004). Woman experience exclusion from ceremonies and important events just because they are infertile. Fear of being divorced or of being separated from their husbands become one of their greatest concerns. Usually the husbands of infertile women are pressurized by their family and friends to remarry. These pressures force the women with infertility to feel isolated and undergo great psychological turmoil (Inhorn, & Balen, 2002). Pakistani women face adverse psychosocial, social, emotional and physical consequences of infertility. Sami and Ali (2006) reported that Pakistani women with infertility experienced mental stress due to 70% physical abuse and 60% of verbal abuse.
Furthermore when a woman is faced with the experience of infertility, it is commonly interpreted as a stressor that needs to be managed. According to Lazarus and Folkman's (1984, as cited in Jordan, & Revenson, 1999) stress and coping theory, cognitive or behavioral coping strategies are used to manage stress, and stress occurs as events in the environment are perceived by an individual to exceed his or her resources.
Along with poor coping women with infertility tend to have self-esteem issues. Rosenberg (1965) theorized self-esteem as positive or negative attitude toward self that is influenced by social and cultural factors (as cited in Mruk, 2006). Self -esteem is what one feels about one's self and how one thinks about one's own selves. It may include one's looks, one's successful relationships with others, one's capabilities and positive attitude toward future (Powell, 2003).
As infertility is referred as a major life stressor so its experience may affect many areas of functioning. One of the main impact infertility has on the women's self-esteem. Female's often report that being diagnosed infertile makes them feel physically defective and it eventually affects its overall body image (Abbey, Andrews, & Halman, 1992).
Quality of life is also impacted when one is stressed: that consists of four major domains. The first domain is physical health in which an individual's overall health is seen: that is how much medical aid one needs, how much energy and capabilities are present in an individual and how much sleep one requires. The second domain is psychological health in which the individual's overall self-esteem and one's religion and beliefs are included. The third domain is social relationships which refer to an impact of social support and sexual activities of an individual. The fourth domain of environment considers the environment of home, freedom, physical safety and security, health and social care (Skevington, Lotfy, & O'Connell, 2003). With its emotionally threatening stressful nature and high cost, infertility is a life crisis for women. It is not only a gynecological illness but also a bio-psycho-social health problem. Generally, infertility has profound psychosocial impacts and it is consistently associated with decreased scores in quality of life (QoL) domains (Beji, & Onat, 2010). Therefore, it can be concluded that addition to the physical implications of infertility, psychological and social functioning may also be disturbed. The stress and loss of child issues involved with infertility also have negative consequences on individual's psychological well-being and overall quality of life.
Participants
The sample consisted of 100 women diagnosed with infertility by gynaechologists. Women with primary and secondary infertility were approached at gyneachological department of public hospitals and private hospitals in Lahore. The women were under treatment since M = 4.70 years. They all were above the age of 25 years
(M = 30; SD = 4.38), married for more than a year (M = 6.94, SD = 4) and under treatment since M = 4.70 years.
Materials and Procedure
To measure the three research variables the participants were asked to complete the following tools:
Coping Strategies Questionnaire: It was developed by Kausar (2001) which consisted of 62 items and was developed for Pakistani population. It was based on which theoretical model proposed by Lazarus. It included four factors: Active practical coping, Active distractive coping, Avoidance focused coping and Religious focused coping with internal consistency reliabilities of 0.72, 0.75, 0.76 and 0.70 respectively (Kausar, 2001). The overall Cronbach alpha reliability of the tool in the present study was 0.87.
The Rosenberg Self-Esteem Scale: It provides measure of global self-esteem. It is made up of 10 items. It refers to self-respect and self-acceptance rated on a 4-point Likert-type scale, ranging from 0 (totally disagree) to 3 (totally agree). The reliability of the tool is 0.87. In present study, Urdu translated version was used after taking permission from the respective author (Ghafoor, & Mohsin, 2011). The Chronbach alpha reliability of the tool in the present study was 0.38.
The WHOQOL-BREF: Urdu version was used in the present study to measure the quality of life of women with infertility (WHOQOL group, 1999). It contains a total of 26 items and has four domains included are general physical health, psychological, social relationship and environment with Chronbach's alpha each domain 0.84, 0.83, 0.84 and
0.83 respectively (WHOQOL group, 1999). In the present study the overall chronbach's alpha calculated was 0.84.
Ethical Consideration
Once the tools were selected for the present research the administrative authorities of hospitals were approached for permissions and help in recruiting the participants. The doctors on duty were assigned the task of referring women who fulfilled the research criteria. The referred participants were then briefed about the aims and objectives of the present study. They were informed that their personal information would be kept confidential and will be used for academic/research purpose only. They were also given the right to withdraw from the research at any point if they wanted to. A total of 120 women were referred, 20 were not included due to either they left before filling all the questionnaires. The participants took averagely 40 minutes to complete the three questionnaires. It took three months to complete the data.
Results
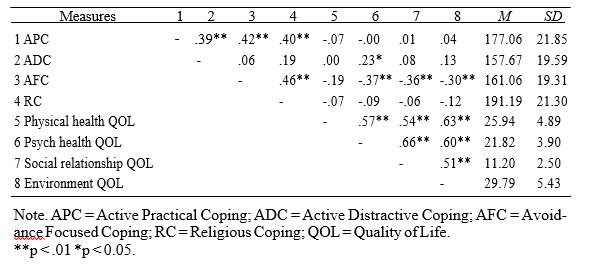
The first analysis result indicated that no significant relationship was found between Active Practical Coping and all domains of Quality of Life. Significant positive correlation was found between Active Distractive Coping and Psychological Health domain of Quality of Life (p <.05). The results further indicated that Avoidance Focused Coping was significantly negatively related with three domains of Quality of Life i.e. Psychological Health (p <.01), Social Relationships (p <.01) and Environment (p <.01). The finding indicated that those infertile women who were using Avoidance Focused Coping showed low scores on their psychological health, social relationships and their environment satisfaction. No significant relation was found between Religious coping and domains of quality of life.
Correlation between Coping Strategies and Quality of Life
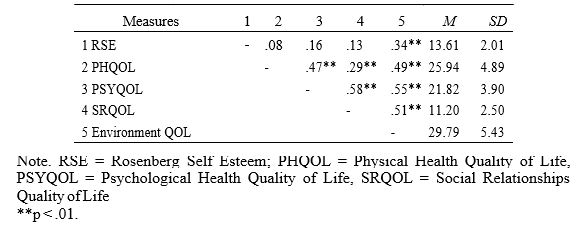
The second set of analysis showed that there was no significant relationship between self-esteem and physical health, psychological health and social relationships domains of quality of life. However there was a significant positive relationship between self esteem and environmental domain of life.
Correlation between Rosenberg Self Esteem and Quality Of Life
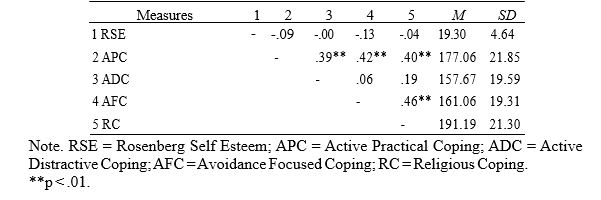
The results showed that there was no significant relationship among the different coping strategies of infertile women and their self esteem.
Correlation between Coping Strategies and Rosenberg Self-Esteem
The experience of infertility is distressing for women. In Pakistani society women's role after marriage is primarily recognized as bearing child. Infertility puts the status of women at stake and they undergo immense stress and make relentless effort to cope with the transitions brought forth by the treatment process, relationship patterns and changing attitude towards life. This study aimed to investigate the relationship of coping strategies, perceived self-esteem and quality of life of women with infertility. The analyses showed some significant relationships of coping strategies with quality of life in all domains.
This highlights that the type of coping determines the quality of life of women with infertility. It was observed that women with Active Distracting Coping reported better psychological health related quality of life. It indicates that those women who adopted adaptive distraction to infertility related distress also tended to have less impairment in psychological functioning. On the contrary, with Avoidance Coping the women reported impaired psychological health, physical health and social relationship related quality of life. A previous study conducted by Davis, Catherine and Dearman (2006) explored the relationship of coping styles of women with their emotional wellbeing. They showed that different coping styles affect overall wellbeing of an individual. A research conducted by Adler and Boxly (1985) concluded that fertile, infertile and formerly infertile patients had no difference in coping styles. Another well supported findings of study by Monga,
Alexandrescub, Katzb, Steinc and Ganiatsd (2003) concluded that being diagnosed as infertile affects the quality of life. They found impaired quality of life reported by women diagnosed with infertility. Hasnain, Abd-El-Raheem and Shahin (2010) concluded that women with infertility reported impaired quality of life and sexual function.
In the present study positive significant relationship was observed between active distractive coping and psychological health domain of quality of life. Whereas avoidance focused coping's relation was found to be negatively significant with three domains of quality of life that are psychological health, social relationships and environment. This showed that those women with infertility who reported avoidance focused coping showed low scores on their psychological health, they had problems in their social relationships and were not satisfied from their environment. According to the latest theory of stress of Lazarus and Folkman (1986), “Psychological stress refers to a relationship with the environment that the person appraises as significant for his or her wellbeing and in which the demands tax or exceed available coping resources” (Lazarus & Folkman 1986, p. 63). According to this theory different individual appraise stress differently and eventually their coping styles are also different. Individuals with better coping skills deal with their problems effectively and take the environment as a challenge. In present study significant positive relationship of Avoidance coping with all domains of Quality of life, inferred that the ineffective coping causes dysfunction in the quality of physical, psychological health, social relationship and interaction with an environment. Another hypothesis regarding the relationship between self-esteem and quality of life of women with infertility was also made. On the whole, according to the results there was no significant relationship between the three domains of quality of life
i.e. physical health, psychological health and social relationship with self esteem. However there was a significant relationship between environment domain and self- esteem. The self-esteem was not observed to be low of the infertile women so it eventually did not affect the quality of life of them. The partial rejection of the hypothesis could be considered due to small sample size. Secondly the women participants may have been denying their problems or could have been defensive. A research conducted by El- Messidi, Al-Fozan, Lin Tan, Farag and Tulandi (2004), investigated that treatment failures of women with infertility affected their quality of life and as in the present study the patients did not encounter any failures regarding their treatments so their self-esteem did not deteriorate which eventually did not affect their quality of life.
Another study conducted by Bringhenti, Martinelli, Ardenti and La Sala (1997) concluded that it is not necessary that every infertile women entering the IVF treatment must show signs of psychological distress. The personality of the infertile woman, her relationship with her husband, her high self esteem and her willingness to adopt a child as the last resort; can eventually help her to deal effectively with her condition and treatment. It is probable that this may have been the case in the present study, as the sample consisted of patients under treatment for infertility that might be the reason of positive self-perception. The third hypothesis was that there would be relationship between coping strategies of women with infertility and self-esteem. The results showed that self-esteem of the sample had no significant relationship with the type of coping strategies they were using. The possible reason could be that the sample was taken from hospitals where proper treatment was available. These women were undergoing treatments and they might be positive regarding themselves and treatment. Secondly, the sample mostly comprised of the females who were married mostly for 10 years, it is likely that the family support has been established substantially during this period.
Thirdly, most of the infertile women informally or formally reported having satisfied relationship with their in laws and husband. This assured that their social support was strong which ultimately helped them in building better and positive image of their selves. The sample included both types of infertility (20 % primary, 80 % secondary), differences of types of infertility could bring useful information on types of coping strategies, level of self-esteem and quality of life. Comparative study needs to be done to explore the differences of women experienced with distress of infertility and coping and quality of life and control with general medical condition or other gynecological condition. Women did not report very low scores on self-esteem. It might be the explicit responses on Rosenberg's Self-esteem questionnaire did not capture the subjective, internalized perception. Qualitative inquiry of phenomenological experiences of women to their infertility diagnosis, distress and impact on their lives will give substantial information to formulate the psychotherapeutic guidelines.
On the basis of the above results it could be concluded that the women with infertility using avoidance focused coping in dealing with infertility related stress experienced impairment in their quality of life in the areas of psychological health, social relationships and adjustment to their environment.
Finding that coping strategies, self-esteem and quality of life are interlinked in women with infertility highlights the intervention implications for such women. Awareness campaign for the women with infertility for the society and the family can be initiated so that the stigma and label could be avoided, so that these women end up having the same amount of respect and care as any other women without any discrimination. These programs need to be initiated in collaboration with the infertility centers and mass media.
Abbey, A., Andrews, F., & Halman, L. (1992). Infertility and subjective wellbeing: The mediating role of self-esteem, internal control and interpersonal conflict. Journal of Marriage and the Family, 54, 408-417. Retrieved from http://www. jstor.org/
Chohan, M. A. (2000). Fundamentals of gynecology. (1st ed.). Pakistan: MAR Publishers.
Daniluk, J. C. (2001). The infertility: Survival guide. USA: New Harbinger Publications, Inc. Retrieved from http://books.google.com.pk/books
Fido, A. (2004). Emotional distress in infertile women in Kuwait. International Journal of F e r t i l e Wo m e n M e d i c i n e , 4 9 , 2 4 - 2 8 . R e t r i e v e d f r o m http://www.ncbi.nlm.nih.gov/pubmed/15038506
Ghafoor, H., & Mohsin, H. (2010). Relationship religiosity, guilt and self esteem in individual's having Obsessive Compulsive Disorder. (Unpublished Master’s thesis.) Centre for Clinical Psychology, University of the Punjab, Lahore.
Husnain, I., M.A., Abd-El-Raheem, T., & Shahin, A. Y. (2010). Primary infertility and health-related quality of life in Upper Egypt. International Journal of Gynecology and Obstetrics, 110 , 118-121. doi:10.1016/j.ijgo.2010.02.015
Hussain, S. (2010). Psychiatric morbidity in infertile Pakistani women. A systematic review. Journal of Pakistan Psychiatric Society, 7 (2), 61. Retrieved from http://www
.jpps.com.pk/display_articles.asp?d=251&p=art
Inhorn, M. C., & Balen, F. (2002). Infertility around the globe: New thinking on childlessness, gender. London: University of California Press, Ltd. Retrieved from http://books.google. com.pk/books
Jordan, C., & Revenson, T. A. (1999). Differences in Coping with Infertility: A Meta-
Analysis. Journal of Behavioral Medicine. 22, 341-358. Retrieved from http://www.ncbi.nlm.nih.go v/pubmed/10495967
Kauser, R., & Munir, R. (2004). Pakistani adolescents' cope with stress: Effect of loss of a parent and gender of adolescents. Journal of Adolescence, 27, 599-610. doi.10.1016/j.adolescence.2003.11.015
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal and coping. New York: Springer Publishing Company, Inc.
Mascarenhas, M, N., Flaxman, S. R., Boerma,T., Vanderpoe, S., & Stevens, G. A. (2012). National, regional, and global trends in infertility prevalence since 1990: A systematic analysis of 277 health surveys. PLoS Med, 9, (12): e1001356. doi:10.1371/journal .pmed.1001356
Mruk, C. J. (2006). Self esteem theory and practice: Toward a positive psychology of self esteem (3rd ed). New York: Springer Publishing Company, Inc. Retrieved from http://books.google.com.pk/books
Mumtaz, Z., Shahis, U., & Levay, A. (2013). Understanding the impact of gendered roles on the experiences of infertility amongst men and women in Punjab. Reproductive Health. 10 (3). doi:10.1186/1742-4755-10-3
Parveen, B., Ahmed, I., Kausar, S., Musharaf , S., Masood, A., & Afzal, S. (2008).
Psychosocial adjustment of educated and uneducated infertile females of Pakistan,2(2),Retrieved fromhttp://www.pmc.edu.pk/Downloads/apmc/apmc_v2n2/11 Psychosocial%20Adjustment%20of%20Educated%20and%20Uneducated%20Inf ertile%20Females%20of%20Pakistan.pdf
Powell, J. (2004). Self-esteem: It's your health. USA: Smart Apple Media. Retrieved from http://books.google.com.pk/books
Reid, J. (2010). An infertility definition to explain primary and secondary infertility. http://ezinearticles.com/?An-Infertility-Definition-to-Explain-Primary-and- Secondary-Infertility&id=4413153
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton, N.J: Princeton
University Press. Retrieved from http://www.emcdda.europa.eu/html.cfm/index 3676EN.html
Sami, N., & Ali, T. S. (2006). Psychosocial consequences of secondary infertility in Karachi. Journal of Pakistan Medical Association, 56 (1), 16-22. Retrieved from http://www.jpma.org.pk/PdfDownload/569.pdf
Sami, N., & Ali, T. S. (2012). Perceptions and experiences of women in Karachi, Pakistan regarding secondary infertility: Results from a community-based qualitative study. Obstetrics and Gynecology International, 108756, 7 .doi:10.1155/2012/108756
Shaheen, R., Subhan, F., Sultan, S., Subhan, K., Tahir, F. (2010). Prevalence of Infertility in a cross section of Pakistani population. Pakistan Journal of Zoology, 42 (4), 389-
Skevington, S. M., Lotfy, M., & O'Connell, K. A. (2004). The World Health Organization's WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial A report from the WHOQOL Group. Quality of Life Research, 13, 299- 310. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/ 15085902le stable/10.2307/353072
World Health Organization. (1999). WHOQOL-Annotated bibliography. Geneva: WHO Publications.