
Cognitive Behavior Management of Insomnia: A Case Study
Adeela Khalid and Nashi Khan, (Ph. D.) Centre for Clinical Psychology
University of the Punjab, Lahore, Pakistan
This case illustrates the Psychological Management of Sleep and Anger Problem with Cognitive and Behavioral Techniques. Assessment was done through Beck Depression Inventory (BDI II) and Sleep Diary. Considering the results of assessment, and complaints, Mr. A.U. (not his true initials) was diagnosed with Insomnia. Psychotherapeutic Intervention was comprised of Cognitive and Behavioral Techniques which showed marked decrease in the symptoms. Improvement was also confirmed by the Psychological Assessment done at Pre and Post Level of therapy.
Keywords: psychological management, cognitive and behavioral techniques, psychological assessment, beck depression inventory, insomnia.
Primary insomnia is a condition of sleeplessness that cannot be attribute to a medical, psychiatric, or environmental reason. Insomnia is quite prevalent, with associated daytime cost of impaired job performance, life quality, and increased risk of co- morbidities including Depression. Insomnia is a frequently reported in one third of the adult population (Morgenthaler et. al., 2006).
The principal symptom according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) is trouble initiating or maintaining sleep, or distress from non-restorative sleep, for at least 1 month. The second criterion is that the sleep trouble (or related day time weariness) sources clinically noteworthy suffering or impairment in social, job-related, or other significant areas of performance. The third condition is that the sleep disturbance not happened exclusively through the course of narcolepsy, breathing-related sleep disorders, circadian rhythm sleep disorder, or a parasomnia. The fourth decisive factor is that the disorder not occurred exclusively during the course of another psychological disorder (e.g., major depressive disorder, generalized anxiety disorder, a delirium). Finally, the fifth criterion is that the trouble is not be due to physiological effects of a substance (e.g., drug abuse, medication) or a general medical condition (American Psychiatric Association, 1994).
The history of client's illness goes back to year 2006. He was preparing for his graduation exams and he used to remain awake whole night and after his exams ended, he was unable to resume his normal pattern of sleeping. He had trouble in falling asleep and remained awake for most part of the night. He reported that he got maximum of 3 hour
sleep and many times in a week he had sleepless nights. This deprivation of sleep caused decline in his academic and later, in his professional performance. He felt stressed and lack of energy. He reported that he got irritated easily and remained worried. When he was unable to sleep, he used to spend time on internet all night. The sleep disturbance remained periodic. He reported that the disturbance in sleep increased whenever he had any stress related to exams, job interviews, job evaluation, and any interpersonal problems with his girlfriend. He also reported that he had a breakup with his girlfriend one month before due to which he felt low and sad. He wanted to marry her but her family was not willing. He missed this relation and in frustration he used to punch the sand bag.
Mr. U.A. belongs to a middle socioeconomic class. His father is 59 years old, lawyer by profession. He is reported to be aggressive and temperamental. His mother is 52 years old, retired as a government school teacher. They are reported to be protective in nature as client being their only son.
Mr. U.A. has three sisters and he is third born. No specific financial stressors reported in the past. He reported sleep walking at the age of 14 years which remained for 1 year on occasional basis. His schooling started at the age of three and a half year. He reported himself to be obedient and average student. He got B grade in Matriculation and Intermediate. He passed his Bachelors Degree with second division and after that he did LLB. He reported to be a social and a regular smoker.
For Formal and Informal Psychological Assessment following scales were administered at Pre, Mid and Post level of Therapy. Informal Assessment was done by taking Subjective Ratings of the Problem, Sleep Diary and Baseline for Anger. Formal Assessment was done by administering Beck Depression Inventory (BDI- II) and Strait Trait Anger Expression Inventory (STAXI).
Showing Score on BDI II at Pre Treatment Phase
|
Scale |
Score |
Category |
|
BDI II |
17 |
Mild |
AXIS I 307.42 Primary Insomnia
AXIS II V71.09 No Diagnosis on Axis II
AXIS III None
AXIS IV Job Related Problem
AXIS V 61-70 (current)
On the basis of Formal and Informal Assessment client was diagnosed with Primary Insomnia. As reported client has difficulty in falling asleep and reported excessive early awakening, with daytime impairment or distress.
The client has predominant complaint of difficulty in initiating sleep. He stays awake at bed for 4 to 5 hours. The sleep disturbance, associated fatigue and headache significantly affect the daily routine. The disturbance is not due to the effect of any substance/drug. The sleep difficulty does not exclusively occur during the course of other sleep disorder (DSM IV, 2000).
A practical model for understanding how insomnia may develop and why it may persist as a chronic condition was first elucidated by Spielman et.al. (1987). Spielman's model (1987), commonly referred to as the “3-P model”, incorporates the impact of various traits (predisposing factors) and life stresses (precipitating factors) in the development of insomnia. It also recognizes that chronic insomnia is maintained (unintentionally) by maladaptive coping strategies (perpetuating factors). Thus, a person may be prone to insomnia due to these maladaptive cognitions. In the case of Mr. U. A.
the predisposing factor was his anxious nature. The exams were considered to be the precipitating factor as well as his maladaptive coping mechanisms like spending time on internet had been maintaining factor for his insomnia.
Management plan comprised of Behavioral and Cognitive Techniques.
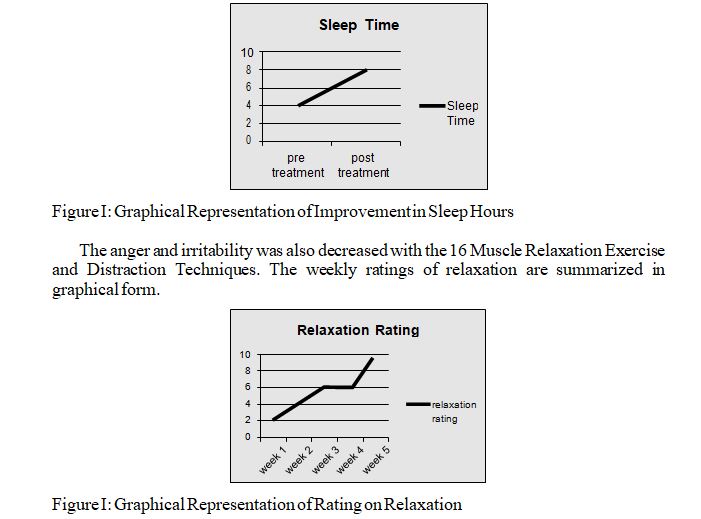
Relaxation Training (16 Muscle Progressive Relaxation Exercise) was used to improve Muscle Relaxation, Sleep and to Decrease the Irritability and Anger. Sleep Hygiene Instruction was used for the systematic process of encouraging those behaviors that optimize sleep quality, while discouraging those behaviors that antagonize sleep. Anger Thermometer and Distraction Techniques was used to deal with the anger outburst of the client in healthy way. Cognitive Restructuring was used to deal with the anger of the client. Thought Replacement Sheet and Evidence For and Against was used for Cognitive Training of the client.
Ten therapeutic sessions were conducted with the client during the course of therapy. Per week one session was conducted.
Below is given a bird eye view of therapeutic sessions.
In first session history of client's problem was taken. In this session the nature, duration and impact of the sleep problem was fully explored. Subjective Ratings were taken around problematic areas. Therapist also explained how therapy will be preceded and the importance of client's active participation in the therapy was emphasized in this session.
In second session, Formal Assessment was done. During this session, the structure of Sleep Management Program was described to the patient. He was told that Psychological Therapy can help to reduce the sleeping tablets quantity and can improve his sleep. An information sheet was provided at the end of the session about Sleep Management Program. Sleep Diary was given to the client for keeping a record of daily sleep.
In third session, the principles of Sleep Hygiene were explained, and any specific contraindicated habits (tea/coffee drinking close to bedtime, inappropriate exercise regimens, etc.) were addressed and discouraged. Guided by estimates of sleep efficiency (i.e. the proportion of time spent in bed asleep) available from the patient's sleep diaries, optimal bedtimes and getting-up times were also proposed in this session, and a target reduction for 'time in bed' was agreed. This sleep restriction aims to reduce the amount of time spent in bed awake, and to align more closely the patient's estimated total sleep time (available from the sleep diary) per night with the amount of time he actually spends in bed.
In fourth session, Sleep Diary was checked by the therapist. Sleep Hygiene instructions were revised in the session. Client was asked to describe how he had incorporated those instructions in his routine and what impact they have caused
According to the client, his sleep quality was improved and the amount of the time spent awake in bed was also reduced. Client was asked to maintain sleep diary and to continue to follow Sleep Hygiene Instructions. Client was then introduced to, and instructed about Progressive Relaxation Technique. Written instructions about Relaxation Exercise were provided at the end of the session. He was asked to take a rating of muscle tension before and after relaxation exercise. He was asked to practice the exercise twice a day.
In fifth session, the information supplied in the Sleep Diary, Sleep Management was reviewed and therapeutic messages from earlier sessions were reinforced. Distraction Techniques were told to the client to deal with is anger in an effective manner. Anger Thermometer was given in order to monitor the level and intensity of his anger and to practice Distraction Techniques at appropriate time. Subjective Ratings on Anger were taken in the session and client was asked to note down the ratings of anger for whole week. Cognitive Errors were identified by providing him a Checklist of Cognitive Errors. Thought Replacement Sheet was explained with example to the client and his Negative Automatic Thoughts were replaced with rational and logical ones in session. Thought Replacement Sheet was also given for home work as well.
Sixth session was started by taking Feedback of previous session from the client. He was practicing distraction techniques and they were helpful for him in managing his anger and irritability. Cognitive Errors were identified by providing him a Checklist of Cognitive Errors. Thought Replacement Sheet was explained with example to the client and his Negative Automatic Thoughts were replaced with rational and logical ones in session. Thought Replacement Sheet was also given for home work as well.
In seventh session, Thought record sheet was reviewed. Client has filled the sheet appropriately. One example from the sheet was discussed in the session. Client experienced anger while using internet as it reminds him of his girlfriend. With the help of therapist, client was made to recognize his cognitive error and replaced dysfunctional thought with functional and rational one.
In eighth session post assessment was done. BDI- II and STAXI was administered for Post Assessment purpose. Sleep Diary was discussed with the client, which showed marked improvement in the sleeping hours of the client. Client managed to sleep 7 to 8 hours per day. He was asked to keep practicing Sleep Hygiene Instructions and 16 Muscle Relaxation Exercise as before on regular basis. The concept of follow up session was introduced to the client.
In ninth session. client was encouraged to come for follow up session for making his progress long lasting. Therapy blue print was provided to the client.
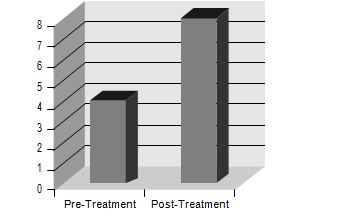
Post Treatment Assessment of the Mr. U.A. had showed that his sleep problem has decreased. Sleep Diary and Sleep Hygiene Instructions proved helpful in dealing with the client's problem. He managed to increase his sleeping hours from 4 hours to 8 hours. The sleep timing is shown in following graph. Due to improved sleep his performance in job was also reported to be satisfactory.
His Cognitive Errors were evaluated and weighed against reality. He was able to identify that he used to minimize positives among his friends and this thing causes problem in his interpersonal relationship. With the help of Thought Replacement Sheet and Anger Thermometer, Mr. U. A. was able to overcome his situational anger and difficulties in interpersonal relationships.
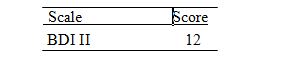
Post assessment results of STAXI and BDI-II are summarized below.
Showing Score on BDI II at Post Treatment Phase
Showing Score on STAXI at Post Treatment Phase
Sub scales Raw score t-score Percentile Interpretation
|
S-Anger |
12 |
54 |
Individual's anger is 85 |
|
|
|
|
|
|
situation ally determine |
|
T-Anger |
15 |
45 |
49 |
Normal Range |
|
T-Anger/T |
6 |
53 |
60 |
Normal Range |
|
T-Anger/R |
6 |
38 |
16 |
Normal Range |
|
AX/In |
12 |
43 |
25 |
Normal Range |
|
AX/Out |
10 |
37 |
10 |
Normal Range |
|
AX/Cont |
12 |
22 |
1 |
Normal Range |
|
AX/EX |
31 |
66 |
87 |
Problems in Interpersonal and at the risk of Medical Disorders |
Insomnia is a common and considerable health concern that is brought about by dysfunctional beliefs regarding sleep, anxiety, and a many sleep-disturbing compensatory practices. CBT tackles these perpetuating factors and has become known as a best treatment choice for Primary Insomnia (Edinger, & Means, 2005). The efficacy of the Cognitive Behavior Therapy has been established for treating insomnia with the help of different well-designed studies. The collective findings of the different studies (Edinger, & Sampson, 2003; Espie, Inglis, Tessier, & Harvey, 2001) have suggested that CBT improves sleep quality, decreases symptoms of depression and anxiety, adjusts dysfunctional beliefs and reduces rely on medications for sleep. Some groundwork data implies that four individual therapeutic sessions conducted at two week intervals may maximize the clinical benefit for the client with insomnia (Edinger, Wohlgemuth, Radtke, & Marsh, 2004).
The CBT has produced improvements in sleep and other problems of the client that have been evaluated subjectively and objectively. There are certain limitations of this case study. Due to the job nature of Mr. U.A. was not able to maintain the follow up sessions. So follow up is recommended for the maintaining improvement gains. The improvement in client's problem was only reported by him subjectively. Objective account could be taken from any family members, who could monitor his sleep patterns and anger out bursts. Large sample size and follow up sessions would help to establish the validity of the findings.
American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental Disorders, Text Revision (4th ed. TR). Washington, DC: American Psychiatric Association.
Beck, A., Brown, G., & Steer, R. (1996). Beck Depression Inventory-II (BDI-II). San Antonio, TX: The Psychological Corporation.
Edinger, J. D., & Sampson, W. S. (2003). A primary care friendly cognitive behavioral insomnia therapy. Sleep, 26, 177–182. Retrieved from http://www.journalsleep.org/ Articles/260209. pdf
Edinger, J. D., Wohlgemuth, W. K., Radtke, R. A., & Marsh, G. R. (2004). Dose response effects of behavioral insomnia therapy: Final report. Poster session to be presented at the annual meeting of the Associated Professional Sleep Societies, Philadelphia, PA. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/17326546
Ellis, A., & MacLaren, C. (1998). Rational emotive behavior therapy: A therapist's guide. St Luis: Impact Publishers.
Espie, C. A., Inglis, S. J., Tessier, S., & Harvey, L. (2001). The clinical effectiveness of cognitive behavior therapy for chronic insomnia: Implementation and evaluation of a sleep clinic in general medical practice. Behaviour Research and Therapy, 39, 45–60. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11125723
Lam, D. (2008). Cognitive Behavior Therapy: A Practical Guide to Helping People Take Control. New York: Routledge.
Lam, D., & Gale, J. (2000). Cognitive behavioral therapy: Teaching a client the ABC model – the first step towards the process of change. Journal of Advanced Nursing, 31(2), 444-451.
Leahy, R. (2003). Cognitive therapy techniques: A practitioner's guide. New York: Guilford Press.
Lim, L., & Nathan, P. (2005). Improving self-esteem. Perth, Western Australia: Center for Clinical Interventions
Miltenberger, R. (1997). Behavior modification: Principles and procedures. New York: Brooks/Cole Publishing Co.