Clinical Management of Frotteuristic Disorder: A Case Study
Anam Maqsood & Mubeena Munir
Department of Applied Psychology, Lahore College for Women University
A 30-year-old male was referred to a mental healthcare institute in Lahore with presenting complaints of deriving pleasure from rubbing or touching a non-consenting person, exhibiting aggressive behavior (such as beating) towards his family members, and irritability. After informal and formal assessment, the client was diagnosed with Frotteuristic Disorder, in a controlled environment. This case was conceptualized using Wolf’s Cycle of Sexual Offending (Wolf, 1984). The management plan for this case was devised according to the behavioral paradigm. A total of 12 sessions were conducted with the client, in which he was given psychoeducation about his problem and the strategies to cope with it. The main technique employed for managing his harassment problem was covert sensitization. For anger management, he was taught relaxation techniques and was also guided about relapse and its prevention. The client reported a significant improvement at the end of therapy.
Keywords: frotteuristic disorder; management; CBT; anger management.
Frotteuristic disorder is a rare and poorly researched paraphilic disorder. This disorder is characterized by recurrent sexual arousal from touching or rubbing against a non-consenting individual. The most common behavior is rubbing or touching one’s genitals against a nonconsenting person or touching another person’s genitals without consent (APA, 2022). It is recommended that people who commit frotteurism should be considered as less aggressive rapists (Horley, 2001). Researchers have also suggested that antisocial behavior and excessive sexual preoccupation may increase the chances of developing this disorder (Wdowiak et al., 2025). In terms of origin, the term frotteurism comes from the French word “frottage”, which means “the act of rubbing”. Krafft-Ebing is credited for explaining this behavior in his book named “Psychopathia Sexualis” in 1886, and Clifford Allen used the term “frotteurism” for the first time in 1969s (Bhatia & Parekh, 2023).
Frotteuristic disorder is a rare and poorly researched paraphilic disorder. This disorder is characterized by recurrent sexual arousal from touching or rubbing against a non-consenting individual. The most common behavior is rubbing or touching one’s genitals against a nonconsenting person or touching another person’s genitals without consent (APA, 2022). It is recommended that people who commit frotteurism should be considered as less aggressive rapists (Horley, 2001). Researchers have also suggested that antisocial behavior and excessive sexual preoccupation may increase the chances of developing this disorder (Wdowiak et al., 2025). In terms of origin, the term frotteurism comes from the French word “frottage”, which means “the act of rubbing”. Krafft-Ebing is credited for explaining this behavior in his book named “Psychopathia Sexualis” in 1886, and Clifford Allen used the term “frotteurism” for the first time in 1969s (Bhatia & Parekh, 2023).
Research shows that frotteuristic behavior is most common in young adolescent males aged 15 to 25 years. Women frotteurs are not common; however, women are the most common targets of frotteuristic behavior, among which both young and older women have been reported as targets (Kafka & Hennen, 2002). In line with this research, another study explains that the prevalence of frotteuristic disorder is difficult to estimate, however, research indicates it occurs predominantly in men, with only a small proportion of women affected (Wdowiak et al., 2025).
A study conducted in Japan showed that young women are the major victims of this crime. There could be a variety of reasons for the prevalence of Frotteurism in Asian countries. These reasons may include the concept of male superiority in Asian culture, the unwillingness of victims to report the crime, an increase in young women's employment, and the sexual frustration of men of all ages. This research also evaluated the prevalence rate of the victims of this disorder from 2002 to 2020 in Japan, India, South Korea, and Sri Lanka. Among these, Japan had the highest range of victims of such acts, i.e., between 24% and 58.1% and Sri Lanka had the lowest rate, i.e., 8% (Kantha & Matsui, 2021). Furthermore, such acts are most likely to occur in a crowded public place, such as public transportation, subways, malls, or elevators, and it has been found that these acts greatly affect the victim’s emotional health (Clark et al., 2016; Fraga Dominguez et al., 2024; Wdowiak et al., 2025).
Regarding the treatment of this disorder, research shows that the treatment is usually sought only after being involved in a criminal activity (Wdowiak et al., 2025). Literature indicates that the successful treatment was achieved through behavioral therapy techniques, which included Jacobson’s progressive muscle relaxation technique, systematic desensitization, and aversion therapy (Kuruvilla & Joseph, 1983). In addition to behavioral therapy methods, two case studies of impulsive frotteurism comorbid with depression reported a gradual decline in the hypersexual behavior of the client after the administration of SSRIs (Fluoxetine, Sertraline) and benzodiazepine (Clonazepam) (Bhatia et al., 2010; Patra et al., 2013). Similarly, another study has suggested that this disorder can be treated effectively through pharmacological treatment along with the therapeutic interventions, including cognitive-behavioral therapy, relaxation exercises, psychoanalytical theory, and solution-oriented therapy (Wdawiok et al., 2025). In line with these studies, the present case study employs a behavioral therapy paradigm to manage symptoms of frotteuristic disorder in a young adult male.
The available literature suggests that research on sexual fantasies and disorders has largely been concentrated in Western countries, with comparatively limited attention given to Eastern and Asian countries. This uneven representation highlights a gap in understanding how sexual fantasies manifest within non-Western societies, where social norms, taboos, and gender expectations differ significantly (Rahim & Soomar, 2021). Research also indicates that paraphilia is a largely underexplored phenomenon, with limited understanding of its etiology, treatment and overall underlying mechanisms (Aggrawal, 2021).
Talking about Pakistan, literature has shown that although sexual violence is a significant concern for Pakistani government and society, there is a lack of reliable data on the prevalence of paraphilic disorders in Pakistan. Evidence suggests that young individuals are more frequently involved in sexual offences, and the cultural norms that encourage the repression of sexual desires may contribute to the manifestation of inappropriate sexual behaviors. The absence of structured sex education for adolescents further limits guidance during critical developmental phases. When combined with experiences of childhood abuse or low self-esteem, these factors may increase the likelihood of sexually offending behaviors (Mustafa & Ali, 2024).
All of the above-mentioned gaps in research and prevalence data highlights the importance of conducting studies on sexual behaviors and paraphilic disorders within the Pakistani context to inform accurate prevalence and culturally relevant understanding and management.
Method
The present study uses an ABA research design in which assessment was done before and after administering behavior therapy to manage frotteuristic disorder.
Case Introduction and Presenting Complaints
A 30-year-old male came to a private-sector mental healthcare institute in Lahore with complaints of deriving sexual pleasure by verbally or physically harassing women (such as touching, rubbing, or grabbing other women without consent), beating family members, and irritability. According to the client, he was educated up to matric, and was unemployed. When he was 22 years old, he started working as a laborer upon his father’s insistence; however, after almost 4 years, he quit working. According to him, he got tired of working and just wanted to hang out with his friends. The client had 3 siblings and was the third-born amongst his siblings. The client’s eldest sibling, his brother, was 37 years old, and as stated by the client, had a satisfactory relationship with the client. However, after he got a job and married, he became busy in his own life and couldn’t give enough time to the client, due to which they didn’t remain that close. The client’s second sibling, his sister, was 34 years old, married, and had 4 children. It was reported by the client’s brother that the client’s relationship with his sister was conflictual, and they used to fight a lot. The client’s youngest sibling was 26 years old, matric qualified, unmarried, and used to work with his father. He had a congenial relationship with the client. The client reported that his general home environment was satisfactory, but a few months back, he started fighting and beating his family on an almost regular basis because his family refused his marriage requests and attempted to prevent his aggressive behavior.
When the client was 15 years old, both of his hands got burnt accidentally in doing some farm-related tasks assigned to him by his father. Gradually, his right hand was completely cured; however, the condition of his left-hand fingers worsened and they had to be amputated. The client’s left-hand fingers amputation was a great shock to the client. In addition to that, his friends and classmates also used to make fun of him. Due to all these reasons, he often felt hopeless, had extremely low self-esteem, and eventually isolated himself. After completing his matriculation, he isolated himself by rarely going out or meeting anyone new. However, when he was 17 years old, he became friends with a group of teenagers who used to verbally harass girls. Those teenagers welcomed him into their group warmly, which made him extremely happy as he felt that there were some of boys of his age who were willing to accept him, regardless of his disability. Regarding his occupational history, he stated that his father got him a job as a laborer when he was 22 years old, but at the age of 26, he quit his job and mostly hung out with his friends.
When the client became friends with the group of teenagers who used to verbally harass girls, he also started to harass girls with his friends, but only verbally. In most cases, the girls used to pass by them quickly without replying. However, in some of the cases, the girls used to retaliate and reply, and some even used to call their male family members, so, in that case, the client and his friends used to flee and make fun of the situation. As time passed, this habit of his became reinforced.
By the age of 28, he started to masturbate very often and harass girls and women physically because his parents were not getting him married. He sometimes used to touch them, grab their arms, or hug them without their permission. As reported by the client, he used to forcefully hug girls so that his chest could rub against theirs, and he used to feel pleasure. After committing these acts, he used to feel guilty, but continued them for pleasure. A few times, he even got slapped and cursed by women whom he had hugged or grabbed, and one time, one of his victims called her brothers who beat him up. Somehow, they also got his house address, went there, and complained to his family. That’s how his family came to know about his actions and tried to stop him.
Onset and Progression
The client’s problem started in 2010 when he was 17 years old, but the symptoms intensified in 2021. Following his left-hand fingers amputation, the client became friends with a group of teenagers at the age of 17. As these teenagers used to harass girls verbally, the client also started to do so. By the age of 27, he started asking his parents to get him married. However, his parents refused since he could hardly earn living. Due to his intense desire and habit of harassing girls, by the age of 28, he started to masturbate very often and harass girls and women physically. He used to touch them in different ways such as by grabbing their arms or hugging them, without their permission, just to obtain sexual pleasure. Initially, the frequency with which he used to perform these activities was low, but with time, and especially from 2021 onwards, the frequency of such acts increased. However, throughout these years, he or his family never sought treatment to manage his issue.
For a period of 3 to 4 months prior to his family seeking treatment, he was extremely irritable, especially whenever his family stopped him from harassing girls. He even used to beat them, and with each passing day, his aggressive behavior worsened. His family got worried for him, and in the last month of 2023, they brought him to a private-sector mental healthcare center in Lahore. After an initial check-up, he was referred to a trainee clinical psychologist for psychological assessment and management.
Assessment
Clinical Interview
Clinical interview is a complex and multi-dimensional interpersonal process which occurs between a professional service provider and the client. Its primary goals are assessment and providing help. Clinicians use information obtained in an initial clinical interview to develop a therapeutic relationship, formulate the case and tailor an appropriate treatment plan (Sommers-Flanagan & Sommers-Flanagan, 2012). A clinical interview was conducted with the client and his brother to gather detailed information about the client and to understand him and his case better. Before the interview was conducted, it was ensured that all of the client’s information would be kept confidential.
Mental Status Examination (MSE)
During the first session with the client, MSE was conducted to evaluate his mental status and current functioning. The client looked like a middle-aged man of average height and was overweight. He had a slouched posture and uncombed hair. He was wearing a dirty and crumpled shalwar kameez. However, he sat on the chair comfortably, maintained adequate eye contact, was responsive, cooperative, and well-mannered. His mood was low, and his affect was consistent with the mood. His rate and tone of speech were normal, he had good articulation, but his volume was low. His orientation of time, place, and person was good. His thought processes were relevant, linear, goal-directed, and coherent. He had no suicidal or homicidal ideation. He had good judgment, abstract thinking, and intellectual ability. He was able to concentrate and had good recent, remote, and immediate memory. No hallucinations and delusions were reported. Insight was present.
Subjective Ratings
The client was asked to rate his symptoms on a 10-point scale, where 0 meant not at all and 10 meant all the time.

Dysfunctional Thought Record (DTR)
Quantitative Analysis

Assessment Measure
Sexual Desire Inventory – 2 (SDI-2)
This scale is used to assess two types of sexual desires, i.e., dyadic desires and solitary desires. Dyadic desire is the desire to engage in a sexual activity with another person. On the other hand, solitary desire is to engage in a sexual activity by oneself and not with others (Spector et al., 1996). It was administered to the client in order to assess his level of sexual desire. The client scored a total of 62 on this inventory; the cut-off score of this inventory is 45, so it meant that the client had more than a normal desire to engage in sexual activities. His responses on this inventory showed that his dyadic desires were much greater than his solitary desires. Based on informal and formal assessment, the client was diagnosed with (F65.81) Frotteuristic Disorder, in a controlled environment (APA, 2022).
Case Conceptualization
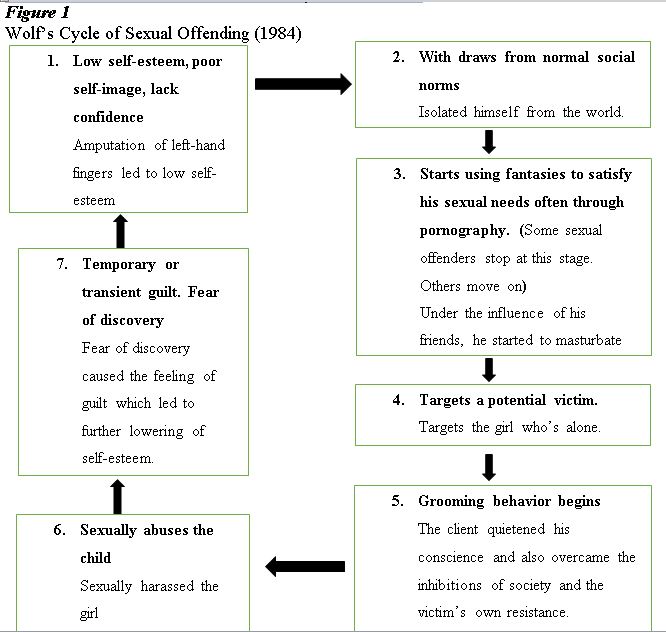
The present case was conceptualized on Wolf’s Cycle of Sexual Offending (1984). According to this model, people who have low self-esteem or who experience rejection from others are the ones who often become sexual offenders. These people suppress their conscience and persuade themselves that no harm will be done if they engage in sexual offending. Initially, they satisfy their sexual needs through fantasies, such as pornography or masturbation. After that, they select a victim, then the grooming behavior begins, during which they get around external restrictions, such as societal rules and the victim’s resistance. In the next step, they sexually abuse the victim, and then due to fear of discovery or feeling of guilt, their self-esteem becomes lowered, and the cycle continues.
Results
The complete amputation of the client’s one-hand fingers lowered his self-esteem, due to which he became hopeless and isolated himself from the world. Then, after establishing a friendship with the boys who used to harass girls, he started to fulfill his sexual desires through masturbation and verbally harassing women. After that, when he asked his parents to get him married, and they refused, his sexual desires intensified. As a result, he started targeting victims, such as girls or women who were alone. Next, he overcame society's restrictions and the victim’s resistance, and physically harassed the victim. Finally, fear of discovery or feelings of guilt lowered his self-esteem, and hence, this cycle continued.
Ethical Considerations
- The client’s sessions were only taken after obtaining his consent.
- The client’s confidentiality was ensured and he was also told about limits of confidentiality.
- The client was treated with utmost respect and compassion.
- The client was actively involved in each session to ensure that the therapeutic process was collaborative and mutual, rather than controlling or directive.


In the first two sessions, the history was taken, and an assessment of the problem was done both informally and formally. In the third session, the diagnosis was finalized, and the client was psycho-educated about the diagnosis, etiological factors, sessions, cognitive behavioral therapy, and the possible outcomes of the treatment. No psychoeducation was provided to the client’s brother because, during treatment, due to some personal issues, he couldn’t visit his brother. Moreover, he also didn’t consent to contact him by phone. In the fourth session, case conceptualization was done through Wolf’s Cycle of Sexual Offending (1984).
During one of the sessions, the client stated that he used to get angry at small things. He recounted an instance when once one of his ward fellows took his pillow without his permission, so he started cursing him loudly. Therefore, in the fifth and sixth sessions, he was taught some relaxation techniques to help him calm down his anger to some extent. These techniques included deep breathing, guided imagery, and taking timeout. The seventh and eighth sessions were focused on challenging the “Overgeneralization” cognitive distortion of the client because the client used to believe that “Everyone hates him” as he once harassed a female employee of that institute by hugging her without her permission. So, in these two sessions, Cost-Benefit Analysis and Behavioral experiment through the Survey method were conducted. In cost-benefit analysis, the client was asked to discuss the pros and cons of his cognitive distortion. In the behavioral experiment, the client was asked to go to different people and ask them about what they think of him after he had told them about the hugging incident.
The next two sessions were centered on dealing with the harassing behavior of the client. In these sessions, the client was taught Covert Sensitization and Assertiveness Training. Covert Sensitization was done in which the client’s behavior of touching girls without their permission was paired with an aversive stimulus of thinking of getting a strong electric shock and feeling nauseous. In the Assertiveness training, the client was taught to communicate his desire to get married to his family more assertively and in more morally appropriate ways. In the last sessions, relapse prevention and post assessment were conducted, and after that, therapy was terminated.
Results
After providing intervention for the client’s complaints, a post-assessment was conducted. These results are shown below.
Subjective Ratings
The client was asked to rate his symptoms on a 10-point scale, where 0 meant not at all and 10 meant all the time.

Dysfunctional Thought Record (DTR)
Quantitative Analysis

Sexual Desire Inventory – 2 (SDI-2)
In post-assessment, the client scored a total of 43 on this inventory, which shows that his desire to engage in sexual activities was within a normal range, as the cut-off score was 45. When compared with pre-treatment results, post-treatment results of SDI-2 show a significant reduction of 19 points.
In this case, the client was suffering from the symptoms of irritability, aggressiveness, and verbally and physically harassing women by touching and hugging them. His symptoms started in 2010, but worsened from 2021 onwards. According to DSM-5-?TR?^TM Frotteuristic Disorder may be diagnosed if recurrent and intense sexual arousal occurs from touching or rubbing against a non-consenting individual for over a period of at least 6 months, as manifested by fantasies, urges, or behaviors (APA, 2022). Moreover, impairment in important areas of functioning may also occur as a result of these urges or when acted upon. As the client’s symptoms were consistent with these criteria, he was diagnosed as suffering from Frotteuristic Disorder.
In his case, the predisposing factor was his school and age fellows making fun of him and not wanting to be his friends, i.e.,a feeling of being alienated. Precipitating factors included the loss of his left-hand fingers, which caused significant distress. His perpetuating factors included guilt and the cognitive distortion that everyone hates him. His protective factors included his family’s support, as evident from their decision to seek treatment for him, and his motivation to improve and become a better family member and person.
Research is scarce in the literature regarding frotteuristic disorder. However, the following are a few perspectives described that are consistent with the client’s case. From the evolutionary perspective of Thornhill and Palmer (2000), the intense sexual desire of males may lead to deviant sexual behaviors. This perspective supports the client’s case, as he had quite a high desire to get married, and when he couldn’t, he started physically harassing women. According to Singer and Toates (1987), sexual activity is not pursued as an escape from pain but rather as an approach to pleasure (Spector et al., 1996). The same thing is reflected in the client’s case, as he used to harass women to gain pleasure.
There is another model that explains the etiology of sexual harassment, i.e., the Four-Factor Model. According to this model, four factors must be present for sexual harassment to occur. These factors include motivation to harass, overcoming internal inhibitions not to harass, overcoming external inhibitions, and overcoming the victim’s resistance (Sbraga & O'donohue, 2000). As seen in the client’s case, he had the motivation to harass women in order to feel pleasure and also overcame the victim’s resistance, his conscience, and society’s rules and regulations to harass women.
The model of the human sexual response by Masters and Johnson (1966) explains that the human sexual response cycle comprises four stages and is pleasurable for the individual. These stages include excitement, plateau, orgasm, and resolution. Kaplan (1979) added another stage before the excitement stage, i.e., the desire stage. During the desire stage, motivation to initiate sexual behaviors is established. Arousal increases during the excitement phase and then intensifies during the plateau phase. The orgasm phase is typically characterized by ejaculation in men and is followed by a return to a non-aroused state in the resolution phase (Ware et al., 2021). This model is also consistent with the client’s case, as the client, before the harassment, had the desire to harass, then his arousal used to increase. Lastly, he used to masturbate and harass women or girls, and feel pleasure.
Conclusion
A total of 12 sessions of approximately 45-50 minutes each were conducted with the client. In the beginning, he was a little hesitant towards the therapy; however, with time, the client became open towards the therapeutic process and followed all the instructions given to him. Especially when his cognitive distortion of Overgeneralizing was challenged and he got to know that nobody hates him but only considers his harassing behavior problematic, he felt relieved and showed greater compliance. By the end of therapy, he became quite active as he started to interact with other people and also participated in group activities voluntarily. Overall, the client showed his determination to get better and reported having significant improvement by the termination of therapy.
Limitations and Suggestions
- The sessions were mostly conducted in places with other clients, fellow trainee clinical psychologists or faculty members present due to lack of a spare room which made the client feel nervous and highly conscious talking about his problems, especially his sexual issues. Therefore, it is suggested that, if possible, future sessions should be carried out in quiet, private and comfortable settings to ensure confidentiality and making the client feel more at ease talking about his complaints.
- On various occasions the client was called for individual or group sessions by the senior psychologist as a part of institutional requirements, disrupting the flow and continuity of the ongoing therapeutic sessions. Therefore, a better coordination between the professionals is suggested to minimize such disruptions.
- The overall therapeutic process was based solely on the client’s self-reported complaints and history; as trainee clinical psychologists were not allowed to contact the family according to the instructional rules. Therefore, it is suggested that psychologists, where possible, include information from the family members or caregivers to gain a more accurate understanding of the client’s history and problems.
- The client was discharged by the mental health facility after 12 sessions; however, there was still a need to work on the guilt feelings of the client.
References
Aggrawal, A. (2021). Unusual Sexual Practices and Sexual Crimes: An Overview. Recent Advances in Forensic Medicine & Toxicology: Volume 3, 335.
Alanko, K., Salo, B., Mokros, A., & Santtila, P. (2013). Evidence for heritability of adult men's sexual interest in youth under age 16 from a population-based extended twin design. The Journal of Sexual Medicine, 10(4), 1090-1099. https://doi.org/10.1111/jsm.12067
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). American Psychiatric Association.
Balon, R. (2016). Frotteuristic disorder. Practical guide to paraphilia and paraphilic disorders, 93-106. https://doi.org/10.1007/978-3-319-42650-1_7
Bhatia, K., & Parekh, U. (2023). Frotteurism. In StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK563260/
Bhatia, M. S., Jhanjee, A., Srivastava, S., & Kumar, P. (2010). An uncommon case of hypersexual behaviour with frotteurism. Medicine, Science and the Law, 50(4), 228-229. https://doi.org/10.1258/msl.2010.010103
Briken, P., Hill, A., & Berner, W. (2003). Pharmacotherapy of paraphilias with long-acting agonists of luteinizing hormone-releasing hormone: a systematic review. J clin psychiatry, 64(8), 890-7. https://doi.org/10.4088/jcp.v64n0806
Clark, S. K., Jeglic, E. L., Calkins, C., & Tatar, J. R. (2014). More than a nuisance: The prevalence and consequences of frotteurism and exhibitionism. Sexual Abuse, 28(1), 3-19. https://doi.org/10.1177/1079063214525643
Cohen, J. S., Edmunds, J. M., Brodman, D. M., Benjamin, C. L., & Kendall, P. C. (2013). Using self-monitoring: Implementation of collaborative empiricism in cognitive-behavioral therapy. Cognitive and Behavioral Practice, 20(4), 419-428. https://doi.org/10.1016/j.cbpra.2012.06.002
Fraga Dominguez, S., Jeglic, E. L., Calkins, C., & Kaylor, L. (2024). Frotteurism and exhibitionism: an updated examination of their prevalence, impact on victims, and frequency of reporting. Journal of Sexual Aggression, 1-18. https://doi.org/10.1080/13552600.2024.2352403
Freund, K., & Seto, M. C. (1998). Preferential rape in the theory of courtship disorder. Archives of Sexual Behavior, 27, 433-443. https://doi.org/10.1023/A:1018796312289
Freund, K., & Watson, R. (1990). Mapping the boundaries of courtship disorder. Journal of Sex Research, 27(4), 589-606. https://psycnet.apa.org/doi/10.1080/00224499009551581