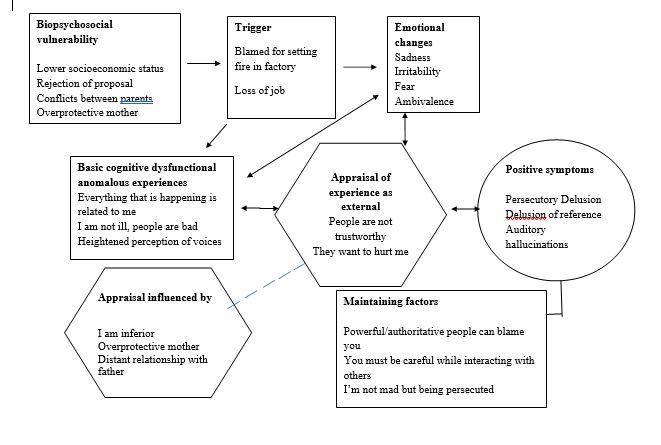
Figure 1
Cognitive Model of Positive Symptoms of Psychosis (Garety et al., 2000)
Intervention
Session 1
- Rapport building
- History taking
- Visual analogue
- Mental Status Examination
- Education
- Feedback and summary of session
- Homework: DTR for delusions, Hallucination Diary
Session 3
- Review Homework
- Family Counselling
- Feedback and summary of session
- Homework: DTR for delusions, Hallucination Diary, Activity Scheduling
Session 5
- Review homework
- Idiosyncratic case conceptualization
- Feedback and summary of session
- Homework: DTR for delusions, Hallucination Diary, Activity Scheduling
Session 7
- Agenda setting
- Hierarchy of situations in which hallucinations are experienced
- ABC model of hallucinations
- Coping Strategies Enhancement
- Feedback and summary of session
- Homework: Use coping strategies enhancement, DTR for delusions, Hallucination Diary, Activity Scheduling
Session 9
- Agenda setting
- Review homework
- Hierarchy of delusions
- Downward arrow technique for delusions
- Behavioral experiment regarding hallucinations
- Feedback and summary of session
- Homework: activity scheduling
Session 11-12
- Agenda setting
- Review homework
Session 2
- Administration of Symptom Checklist- R
- Feedback and summary of session
- Homework: DTR for delusions, Hallucination Diary, Activity Scheduling
Session 4
- Review Homework
- Socialization
- Feedback and summary of session
- Homework: DTR for delusions, Hallucination Diary, Activity Scheduling
Session 6
- Review homework
- Socialization
- Progressive Muscle Relaxation
- Feedback and summary of session
- Homework: DTR for delusions, Hallucination Diary, Activity Scheduling
Session 8
- Agenda setting
- Review homework
- Generating list of idiosyncratic distraction techniques
- Evidence for and against
- Feedback and summary of session
- Homework: activity scheduling
Session 10
- Agenda setting
- Review homework
- ABC model of delusions
- Feedback and summary of session
- Homework: activity scheduling
Session 13-14
- Agenda setting
- Review Homework
- ABC model of delusions
- Evidence for and against delusion
- Feedback and summary of session
- Homework: activity scheduling and mastery and pleasure
Session 15
- Agenda setting
- Review homework
- Assertiveness training
- Relapse prevention (Therapy Blueprint)
- Behavioral experiment for challenging delusions
- Feedback and summary of session
- Homework: activity scheduling and mastery and pleasure
Session 16
- Post assessment
- Mental Status Examination
- Visual Analogue Scale
- Symptom Checklist -R
- Feedback and summary of session
Results
After management of the client’s complaints, post-assessment was done. The results of the post-assessment are shown below.
Visual Analogue
The client was asked to rate his symptom once a week on a 10-point scale where 0 meant no symptoms and 10 meant severity.
Table 2
Showing Pre and Post Assessment Ratings of Presenting Complaints
|
Symptoms |
Pre-Treatment |
Post Treatment |
|
Suspiciousness |
9 |
3 |
|
Hearing voices |
9 |
4 |
|
Anxiousness |
10 |
4 |
|
Restlessness/ pacing |
9 |
4 |
|
Social Withdrawal |
10 |
3 |
Symptom Checklist-R (Rahman et al., 2009).
After the completion of therapy, the Schizophrenia subscale of Symptom Checklist-R was re-administered and the participant scored 24 on the scale. The obtained score was below the mean (M=26, SD=13) and showed a significant decrease in the symptoms of schizophrenia.
Discussion
In the present case, client was experiencing auditory hallucinations, referential delusions and persecutory delusions. Client’s level of functioning in work, interpersonal relationships and self-care was also markedly impaired. According to DSM-5 (APA, 2013), at least two symptoms must be present for a significant portion of time during a 1-month period or longer. At least one of these symptoms must be the clear presence of delusions, hallucinations, or disorganized speech. Grossly disorganized or catatonic behaviour and negative symptoms may also be present. Schizophrenia also involves impairment in one or more major areas of functioning. The symptoms of the client were consistent with the diagnostic criteria of Schizophrenia.
In the present case, client’s predisposing factors were his low socio-economic status, conflicting relationship between parents and overprotective mother. Kohn (as cited in Kring et al., 2012) explained that higher rates of schizophrenia are found in people of the lowest socioeconomic status (SES). It may be due to low levels of education, lack of rewards and opportunities when taken together with low SES make people predisposed to develop schizophrenia. It is evident in the present case as the client belonged to lower socio-economic status and was educated till secondary. According to Comer (2013), parents of people with this disorder often (1) display more conflict, (2) have greater difficulty communicating with one another, and (3) are more critical of and overinvolved with their children than other parents. It can be observed in the present case, as client’s parents always had conflict with each other and had difficulty communicating with each other. His mother was also critical and was overly involved with client and his siblings.
According to Beck et al. (2009), traumatic events can result in the formation of delusions and hallucinations. In the present case, client’s first episode was triggered when he was blamed for setting fire at his workplace and lost his job. From that time, he was conscious of not making any mistakes. According to the cognitive explanation (Tarrier, 2008, as cited in Comer, 2013), symptoms of schizophrenia are triggered when an individual attempts to understand their unusual experiences. When an individual first confronts the voices, they turn to friends and relatives, who deny the reality of these sensations, and eventually, the sufferers conclude that the others are hiding the truth from them. They begin to reject all feedback and some develop beliefs (delusions) that they are being persecuted. It is evident in the present case, the client discussed these experiences with mother who denied it and then the client felt that she was trying to reject him and resulted in delusions.
Client’s maintaining factors were his biased thinking, safety behaviours and the high expressed emotions in family. Beck et al. (2009) also reported that clients with delusions, especially persecutory delusion often use a number of safety behaviours in an attempt to avoid or neutralize danger. In the present case, client’s safety behaviours were ‘not looking here and there’ and ‘not talking to anyone’. Similarly, Beck et al. (2009) explained biased thinking for the analysis of delusions. They proposed that they have egocentric orientation that pre-empts normal information processing in favour of self-referential attributions of irrelevant events. Depending on the content of this self-centred orientation, these clients unrealistically perceive themselves as the central focus of others’ attention. The central feature of the biased thinking is the indiscriminate attribution of negative or positive intentions to other people. In the present case, client was thinking that if people are laughing, they are laughing at me and people are not trustworthy.
Client’s maintaining factors were the high expressed emotions in family. Families who are high in expressed emotions i.e. members frequently express criticism, disapproval, and hostility towards each other and intrude on one another’s privacy. Further, it was reported that individuals who are trying to recover from schizophrenia are almost four times more likely to relapse if they live with such a family than if they live with one low in expressed emotion (Bebbington & Kuipers, 2011, as cited in Comer, 2013). In the present case, the client was living in environment with high expressed emotions. Garety et al. (2000) proposed that biopsychosocial vulnerability along with life events, adverse environments, illicit drug use, or periods of isolation lead to emotional changes, and disruptions in cognitive processes of attention, perception, or judgement which ultimately lead to delusional beliefs and hallucinations. These factors were maintaining the symptoms of client.
Conclusion
Client remained in treatment for approximately two months and showed compliance towards therapy. In the beginning, the client was resistant and it was difficult for him to understand that he was distressed by the appraisal of hallucinations and delusions rather than the voice itself. With time, client learnt that the voice has no control over him and people are not against him. Client reported that he benefitted most from verbal challenging technique i.e., evidence for and against. He also reported that mastery and pleasure chart helped in motivating him for work. At the time of termination, client reported significantly less number of hallucinations and degree of conviction on delusions also decreased. His pacing and restlessness was significantly improved and he also started talking to other people at work. Overall, 70 % improvement was observed.
Limitations and Suggestions
- There is a need to work on the evaluative beliefs of the client which would further help client in reducing the chances of relapse and it would help client in improving his beliefs regarding
- Follow up sessions are also suggested to further check the maintenance of therapeutic
References
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). American Psychiatric Association.
Beck, A. T., Rector, N. A., Stolar, N., & Grant, P. (2009). Schizophrenia: Cognitive theory, research, and therapy. The Guilford Press
Brabban, A., Tai, S., & Turkington, D. (2009). Predictors of outcome in brief cognitive behavior therapy for schizophrenia. Schizophrenia Bulletin, 35(5), 859–864. http://doi.org/10.1093/schbul/sbp065
Comer, R. J. (2013). Abnormal psychology (8th ed.). USA: Worth Publishers.
Ganguly, P., Soliman, A., & Moustafa, A. A. (2018). Holistic Management of Schizophrenia Symptoms Using Pharmacological and Non-pharmacological Treatment. Frontiers in Public Health, 6, 166. http://doi.org/10.3389/fpubh.2018.00166
Garety, P. A., Kuipers, E., Fowler, D., Freeman, D., & Bebbington, P. E. (2001). A cognitive model of positive symptoms of psychosis. Psychological Medicine, 31, 189-195. http://doi.org/10.1017/s0033291701003312.
Gejman, P. V., Sanders, A. R., & Duan, J. (2010). The role of genetics in the etiology of schizophrenia. The Psychiatric Clinics of North America, 33(1), 35–66. http://doi.org/10.1016/j.psc.2009.12.003
Gould, R. A., Mueser, K. T., Bolton, E., Mays, V., & Goff, D. (2001). Cognitive therapy for psychosis in schizophrenia: An effect size analysis. Schizophrenia Research, 48, 335–342. http://doi.org/10.1016/S0920-9964(00)00145-6
Henriksen, M. G., Nordgaard, J., Jansson, L. B. (2017). Genetics of schizophrenia: overview of methods, findings and limitations. Frontiers in Human Neuroscience, 11, 332. http://doi.org/10.3389/fnhum.2017.00322
Kring, M. A., Johnson, S. L., Davison, G. C., & Neale, J. M. (2012). Abnormal psychology (12th ed.). John Wiley & Sons
Naqvi, I., Murtaza, M., Nazir, M. R., & Naqvi, H. A. (2010). Gender difference in age at onset of schizophrenia: a cross sectional study from Pakistan. Journal of Pakistan Medical Association, 60(10), 886-889
Rahman, N. K., Dawood, S., Rehman, N., Mansoor, W., & Ali, S. (2009). Standardization of Symptom Checklist –R on Psychiatric and Non Psychiatric amole of Lahore City. Pakistan Journal of Clinical Psychology, 8(2), 21-32
Rector, N. A. & Beck, A.T. (2001). Cognitive behavioral therapy for schizophrenia: An empirical review. The Journal of Nervous and Mental Disease, 189(5), 278–287. http://doi.org/10.1097/00005053-200105000-00002
Wykes, T., Steel, C., Everitt, B., & Tarrier, N. (2008). Cognitive behavior therapy for schizophrenia: effect sizes, clinical models, and methodological rigor. Schizophrenia Bulletin, 34(3), 523–537. http://doi.org/10.1093/schbul/sbm114
Zimmermann, G., Favrod, J., Trieu, V. H., & Pomini, V. (2005). The effect of cognitive behavioral treatment on the positive symptoms of schizophrenia spectrum disorders: a meta-analysis. Schizophrenia Research, 77(1), 1-9.
http://doi.org/10.1016/j.schres.2005.02.018
Zubin, J., & Spring, B. (1977). Vulnerability: a new view of Schizophrenia. Journal of Abnormal Psychology, 86,103-126. http://doi.org/10.1037//0021-843x.86.2.103
Contribution of Authors
|
Sr. No. |
Author |
Contribution |
|
1. |
Mubeena Munir |
Conducting Sessions, Manuscript Writing |
|
2. |
Fakhra Wakil |
Pre and Post Assessment, Review of Manuscript |