Posttraumatic Stress Disorder and Posttraumatic Growth: Two Realities among Flood Affected School Going Children in Pakistan
Nazia Bashir
University of the Punjab, Lahore, Pakistan
Rukhsana Kausar
Government College Women University, Sialkot, Pakistan
Nashi Khan
Rashid Latif Khan University, Lahore, Pakistan
The present study tended to study the relationship between posttraumatic stress disorder (PTSD) and posttraumatic growth (PTG). It also covers the predictive role of demographic features and flood-related experiences for PTSD and PTG in school children living in the flood-prone area of Southern Punjab, Pakistan. 273 school going children were assessed in 2016 after one year to expose flood. Urdu version of Posttraumatic Growth Inventory for Children –Revised, Child PTSD Symptom Scales and demographic form were used to assess PTG and PTSD respectively in children falling in the age range of 11-17 years. The devastation of the school building and financial loss in form of crop damage were the positive predictors of PTSD. Moreover, living in tents, the experience of homelessness, financial losses, exposure to wounded and dead bodies, education, and occupation of the father were noteworthy indicators of PTG. No relationship was noted between PTSD and PTG. Findings supported the notion that PTSD and PTG can coexist therefore clinical implications and ideas related to preventive planning are discussed.
Keywords: post-traumatic stress disorder (PTSD), demographic, flood-related variables and post-traumatic growth (PTG).
Before adulthood emerges, nearly 80% of children and adolescents go through a certain type of trauma (Ghazali et al., 2014; Southwick et al., 2014) and may experience symptoms of PTSD including re-experiencing, avoidance, negative cognitions, and arousal (APA, 2013). The risk of getting a diagnosis of PTSD increases if a child or adolescent exposed to natural catastrophe (Goenjian et al. 1998; Lonigan et al. 1994). However, recent literature suggests that post-traumatic growth (PTG) is also prevalent amongst children and adolescents who survive such disasters (Dekel et al., 2012; Linley et al., 2003; Tedeschi & Calhoun, 2004). As a result of PTG, survivors develop an optimistic attitude, learn, and experience positive psychological changes following a detrimental traumatic event (e.g., Tedeschi & Calhoun, 2004).
Currently, researchers have shifted their attention to the positive aspect of trauma like PTG in trauma studies. They have begun to analyze the link between PTG and PTSD. Some of them concluded that individuals experience greater PTG when they have experienced severe PTSD (Helgeson et al., 2006; Lehman et al., 1993; Park et al., 1996; Tomich & Helgeson, 2004; Laufer & Solomon, 2006; Solomon & Dekel, 2007), whereas, others demonstrated that PTG can also be experienced with fewer symptoms of PTS (Ai et al., 2005; Frazier et al., 2001; Hall et al., 2008; McMillen et al., 1997). On the other hand, some also supported the view that PTG is not related to psychological disturbance (Cordova et al., 2007; Val & Linley, 2006; Widows et al., 2005). It has been argued that variations among the findings of trauma studies might be because of different factors that correlate with the process of PTG and PTSD (Helgeson et al., 2006).
Contributing factors including early age (Southwick et al., 2014), gender, education, marital status, ethnicity along with disaster-related stressors are associated with greater levels of PTG and PTSD (Wang et al., 2013; Brewin, Andrews, & Valentine, 2000; Xu & Liao, 2011). After experiencing natural disasters the intensity of the traumatic event, the distress caused by the event and the enduring time since the traumatic event (Linley & Joseph, 2004; Lindstrom & Triplett, 2010), the loss of loved ones (Xu & Liao, 2011), psychological functioning at pre and post-disaster (Weems et al., 2007; Lowe et al., 2013) seem to relate to different levels of PTG as well as PTSD.
In Pakistan despite the growing interest of the researchers in investigating the outcome of a traumatic experience, there is still a shortage of literature on the experiences of children exposed to natural disasters. However, 45% population of Pakistan based on children (adolescent group). Thus, the current study intends to add to the existing research by finding the association between PTG and PTS symptoms in flood survivors children aged 11-17 years, lived in Southern Punjab, Pakistan. Furthermore, it examines the predictive role of demographic and flood-related variables for PTSD and PTG that could affect the process of mental health in so many ways in children exposed to a flash flood.
Method
Research DesignThe cross-sectional correlation study was executed in flood-prone villages of Muzaffargarh District of South Punjab, Pakistan.
SampleData of 273 children ranging from 11-17 years of age (M=13.61 years and SD = 1.76) was taken through purposive sampling from 6 government schools in 2016. Only those children were recruited who were exposed to flood at least one time in their lives and had no other traumatic experience in the previous six months.
Measures
Demographic Information FormThe demographic information form was set by the researchers after an extensive review of the literature. It included essential details about the participant including their age, sex, schooling, religion, parental education, and occupation along with the nature of flood-related experiences that they went through. To assess responses on flood-related experiences (e.g., get physical disability, living in tents, had financial losses in form of loss of crops/ damage of lands, loss of cattle/fish forms, damage or devastation of home and schools, had emotional trauma in form of witnessing wounded, dead bodies and death of closed one, etc.) they were asked to respond on each item with response option a) Had no such experience; b) Closely experienced such suffering at home level; c) Experienced suffering at others level other than family members; d) Experienced suffering at above both levels (family as well as other people around). During analysis, the highly responded category of each item was taken as the baseline group in dummy coding. effectiveness in the workplace which ultimately accounts for organizational progress. Laschinger and Finegan (2005) investigated that SE has a positive impact on EE.
Child PTSD Symptom Scale- V (CPSS-5; Foa & Tolin, 2000)The CPSS-V was based on the PTSD criteria of DSM 5. Its purpose was to examine whether or not the child has experienced any specific alarming indication last month. It is measure of 27 items. Its initial 20 items are related to PTSD symptoms with a 5 point (0-4) Likert scale where ‘0’ means not at all and ‘4’ means six or more times a week/severe’ and the last 7 items are related to general daily functioning that are rated on yes / no scale. 31 score was considered as an indicator of PTSD in the child. Initially, it was translated into the Urdu language by the researcher before using it in the field. It was appeared to be highly authentic with Cronbach's alpha = 0.84 for the present study.
Posttraumatic Growth Inventory for Children -Revised (PTGI-C-R; Kilmer, Gil-Rivas, Tedeschi, Cann, Calhoun, Buchanan, and Taku, 2006)Urdu translated version (Liaqat & Rukhsana, 2007) of PTGI-C-R was used to examine the positive changes occurring in the children’s behaviors after exposing the flood. The 10 items questionnaire has a 4-point scale (1– 4) to measure PTG. Moreover, Cronbach's alpha was .67 for the current sample.
Procedure
Ethics research committees i.e., Departmental Doctoral Program Committee of Centre for Clinical Psychology, University of the Punjab and University Advanced Studies Review Board of University of the Punjab, Lahore, Pakistan approved the study. Permission was sought out from the authors to use their tools in the present study. Then, a Pilot study was executed on a sample of 10 participants of the same age to assess their comprehension and conceptual clarity of the items. No revisions were made in the questionnaire’s responses. Schools located in flood- prone areas were approached. School authorities were briefed about the nature of the research and permission was taken to collect data. Later, all self-report questionnaires were completed in groups in their class setting.
Ethical ConsiderationWhile conducting the study efforts were made to follow the ethics of the research. Permissions related to use tools and to collect data were sought out from respective authorities. Not only participants but also school authority was well informed about the purpose, procedure of study, role, and rights of the participants. They were also briefed about the confidentiality of their information and results.
Results
The Statistical Packages for Social Sciences- version 21 (SPSS-21) was used to analyze the data. Correlation among demographic variables and study variables was carried out through Pearson Product Moment Correlation. The results revealed non-significant relationship between PTSD and PTG. The age of participant had a significant positive relationship with the PTG. Girls experienced more PTSD symptoms (r = .14, p =.01) than boys (See Table 1 for details).
Table 1 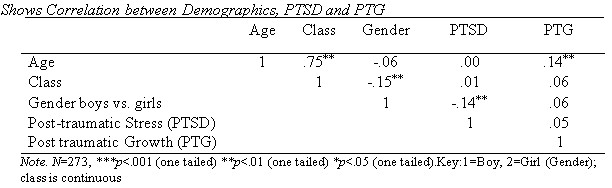
One-way multivariate analysis of variance (MANOVA) was carried out to see the mean differences between different categories of flood related variables on PTSD and PTG. The results of MANOVA analysis also showed that there are significant mean differences on the scores of PTSD and PTG for participants’ father’s education as evident by the model F (18, 524) = 1.877, p = .016; Wilks’ Lambda = .883; partial eta squared = .06. The analysis also showed significant mean differences due to father’s occupation F (18, 524) = 1.80, p = .022; Wilks’ Lambda = .886; partial eta squared = .05.
Participants who were homeless showed significant differences between the mean scores, F (27, 762.89) = 1.73, p = .012; Wilks’ Lambda = .84; partial eta squared = .05. On the other hand, participants who were living in tents also showed significant differences on PTSD and PTG as evident by F (27, 762.89) = 1.66, p = .019; Wilks’ Lambda = .846; partial eta squared = .05. Similarly, participants who experienced loss of crops also performed differently on the mean scores of PTSD and PTG F (27, 762.89) = 2.29, p < .001; Wilks’ Lambda = .796; partial eta squared = .07.
MANOVA also showed that devastation of school building also significantly impacted the scores of participants on PTSD and PTG, F (27, 762.89) = 2.53, p < .001; Wilks’ Lambda = .778; partial eta squared = .08. Additionally, participants who witnessed wounded and witnessed dead bodies also showed significant differences between the mean scores of PTSD and PTG. As explained by the model, F (27, 762.89) = 3.35, p < .001; Wilks’ Lambda = .720; partial eta squared = .10, for witnessing wounded. For witnessing dead bodies, the model reporting was F (27, 762.89) = 2.07, p < .001; Wilks’ Lambda = .813; partial eta squared = .06, depicting the significant differences among participants on the scores of PTG.
Table 2 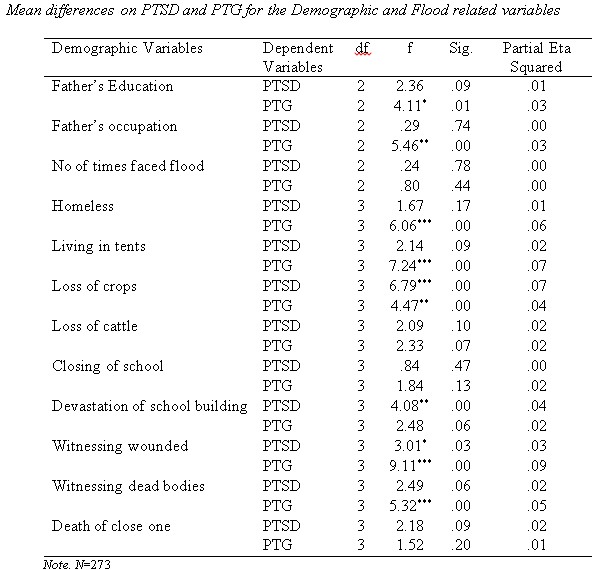
Later, significant demographic and flood related variables obtained by correlation and MANOVA analysis were used in performing Multiple Regression analysis (step wise) to determine the predictors of PTSD and PTG. The regression analysis revealed that the overall ∆R2 model of PTSD was significant and 9% variance was explained with F (4, 268) = 8.08, p < 001. It revealed that experiencing the devastation of a school building at personal vs. other level and lose of crops at personal vs. others; personal vs. no loss and personal vs. all level were significant predictors of PTSD in children.
Table 3 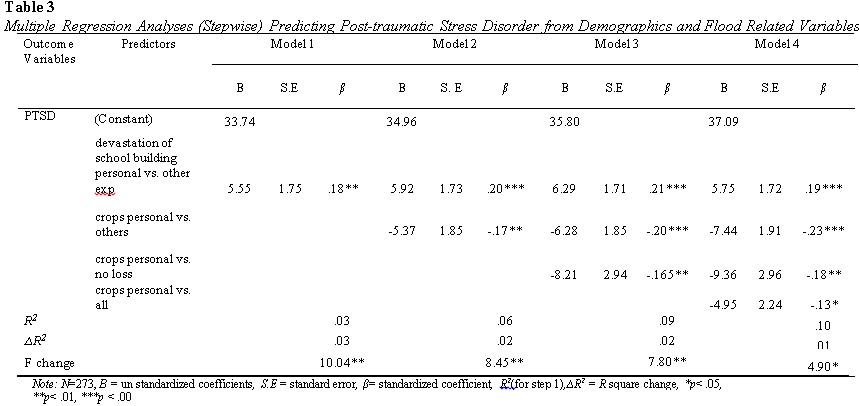
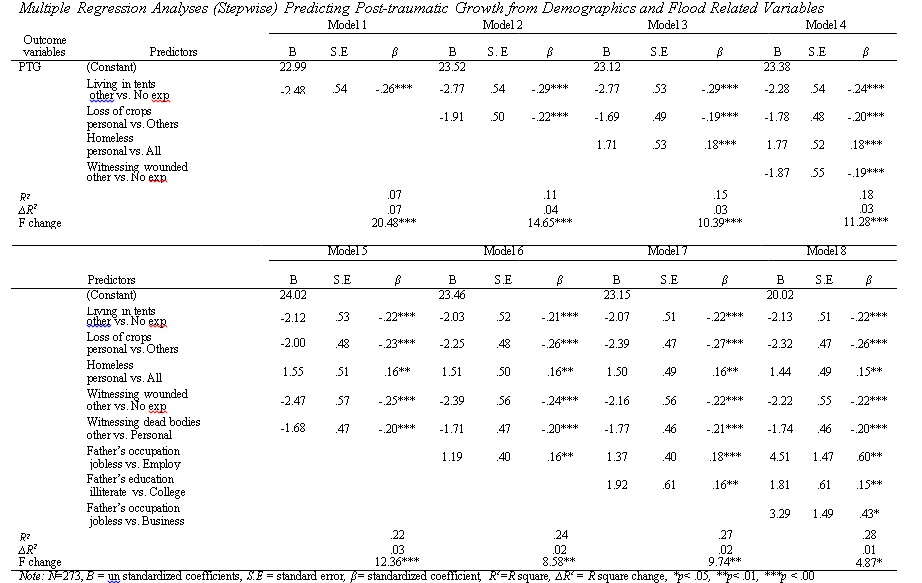
∆R2 model of post-traumatic growth was also found significant and 26% variance with F (8, 264) = 13.19, p < 001 was explained. Experience of living in tents other vs. having no such experience, loss of crops personal vs. others, homelessness at a personal level vs. all, witnessing wounded at other levels and witnessing dead body other vs. personal were significantly predicted the post-traumatic growth of trauma survivors. Similarly, the employment status of the father and education up to college also significantly predicted post-traumatic growth among survivors of natural disasters.
Discussion
The study aims to explore the link between PTSD and PTG along with identifying the shared and unique demographic and flood-related predictors for PTSD and PTG that could affect the process of recovery in flood survivor children of Southern Punjab, Pakistan.
The finding revealed that overall PTSD did not appear significant for the total PTG. However, it appears that positive learning comes forward from distress. It might be due to in case of facing major life crises person develops a sense of struggle to seek opportunities to provide him a better future. Furthermore, it seems like in fighting with PTSD symptoms one probably shifts his/her attention to think about the meaning of life in a positive sense. In the long run, it will help him/her to increase the sense of strength.
These results are in line with other research evidence (e.g., Levine et al., 2008; Karenci et al.,2012; Cieslak et al., 2009). The presence of PTSD and PTG in school going children is more pronounced when we see it in the context of participants’ religion. All were Muslims and shared the general understanding that suffering and distress are part of life and could potentially yield positive change. Evidence suggested that when one positively holds the trauma-related information while facing a traumatic event and incorporates earlier beliefs psychological growth can happen during hardship (Joseph & Linley, 2005).
Further, the results revealed that experiencing financial loss in form of damage to crops can develop PTSD. Those who experienced the devastation of schools also experienced PTSD. The findings are also consistent with the prior literature such as Nygaard and Heir (2012) studied the aftermaths of the tsunami and suggested that the material losses suffered due to natural disasters may cause psychological distress and reduced quality of life (Nygaard & Heir, 2012; Kraemer et al, 2009).
The results also revealed that those who had exposure to dead bodies, wounded, and experienced homelessness or living in tents also experienced PTG. Participants whose father was educated and employed also learned to practice post-traumatic growth after the trauma. A plausible reason for this finding could be that loss of a source of income and poor social resources has been associated with poorer psychological health after a trauma (Kumar et al., 2007) and early financial stability and social recovery could lead the children to reflect on the experience of trauma and develop PTG.
Evidence suggested that PTSD was higher among females (Kumar et al., 2007). The current study also reported similar results that girls were prone to experience PTSD. Few studies provide a reason for more reported symptoms of PTSD by females as compare to males could be that females may have experienced more inequity, harassment, and dependency during such traumatic incidents (Wolfe et al., 1999). Therefore, future studies should cover a wide range of possible traumatic experiences in both sexes while exposing huge catastrophes.
Study Limitation
The present study has some shortcomings including based on a cross-sectional design, execution in rural areas, and while getting data to use only self-report measures. Due to these limitations, findings are not generalizable and causal inferences cannot be drawn from them. Thus, the future investigation would advantage from mixed-method longitudinal research design to fully explore post-trauma outcomes in a culture-sensitive context. Individual interviews of survivors having PTSD along with self-report measures could flourish more rich findings. Moreover, parental history of PTSD, stress tolerance, level of PTG, and parental post-trauma behaviors could be informative demographics for advanced study in the field of trauma.
Clinical Implication
The participants of this study lived in a flood-prone area and witnessed a flood many times at a young age. They are used to face aftermaths of disaster and well aware of the bitter realities of their life, despite that PTSD is still present in this sample and they also display the positive change in them. At this point, there is a need to prepare material on psycho-education of PTSD and to promote PTG that could be used at the preventive level in Pakistan. Clinicians should be taken seriously, as it is a need of time to promote healthy mechanisms in the response to adversity. The findings help them to increase their efforts to develop culturally appropriate treatment manual based on techniques that convert patient’s attention from the distress of experience to the meaning of experience and apply the intervention to reduce the risk of PTSD otherwise this could appear as a lifelong burden for children and adolescents of Pakistan.
Conclusion
The current study involved children who exposed to flood and enlighten the understanding that healthy transformation happens in the aftermath of devastation. However, PTG and PTSD are not found to be overlapped construct as different factors predict the likelihood of each e.g., paternal education or occupation, to see others getting shelter in tents, wounded people around and homelessness are predicting PTG; whereas, the devastation of the school building is found to be PTSD predictors. The study also uncovered the shared predictors of PTSD and PTG such as experiencing financial loss inform of crops. Thus, survivors should be educated about the manifestation of PTSD symptoms and the constructive site of PTG at the preventive level.
References
Ai, A. L., Cascio, T., Santangelo, L. K., & Evans-Campbell, T. (2005). Hope, meaning, and growth following the September 11, 2001, terrorist attacks. Journal of Interpersonal Violence, 20(5), 523–548. https://doi.org/10.1177/0886260504272896
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Brewin, C. R., Andrews, B., & Valentine, J. D. (2000). Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. Journal of Consulting and Clinical Psychology, 68(5), 748–766. https://doi.org/10.1037//0022-006x.68.5.748
Cieslak, R., Benight, C., Schmidt, N., Luszczynska, A., Curtin, E., Clark, R. A., & Kissinger, P. (2009). Predicting posttraumatic growth among Hurricane Katrina survivors living with HIV: the role of self-efficacy, social support, and PTSD symptoms. Anxiety, Stress, and Coping, 22(4), 449–463. https://doi.org/10.1080/10615800802403815
Cordova, M. J., Giese-Davis, J., Golant, M., Kronenwetter, C., Chang, V., & Spiegel, D. (2007). Breast cancer as trauma: Posttraumatic stress and posttraumatic growth. Journal of Clinical Psychology in Medical Settings, 14(4), 308–319. https://doi.org/10.1007/s10880- 007-9083-6
Dekel, S., Ein-Dor, T., & Solomon, Z. (2012). Posttraumatic growth and posttraumatic distress: A longitudinal study. Psychological Trauma: Theory, Research, Practice, and Policy, 4(1), 94–101. https://doi.org/10.1037/a0021865
Foa, E. B., & Tolin, D. F. (2000). Comparison of the PTSD Symptom Scale-Interview Version and the Clinician-Administered PTSD scale. Journal of Traumatic Stress, 13(2), 181–191. https://doi.org/10.1023/A:1007781909213
Frazier, P., Conlon, A., & Glaser, T. (2001). Positive and negative life changes following sexual assault. Journal of Consulting and Clinical Psychology, 69(6), 1048– 1055. https://doi.org/10.1037/0022-006X.69.6.1048
Ghazali, S. R., Elklit, A., Balang, R. V., Sultan, M. A., & Kana, K. (2014). Preliminary findings on lifetime trauma prevalence and PTSD symptoms among adolescents in Sarawak Malaysia. Asian Journal of Psychiatry, 11, 45– 49. https://doi.org/10.1016/j.ajp.2014.05.008
Hall, B. J., Hobfoll, S. E., Palmieri, P. A., Canetti-Nisim, D., Shapira, O., Johnson, R. J., & Galea, S. (2008). The psychological impact of impending forced settler disengagement in Gaza: trauma and posttraumatic growth. Journal of Traumatic Stress, 21(1), 22–29. https://doi.org/10.1002/jts.20301