
*Alina Shahid
Centre for Clinical Psychology, University of the Punjab
Department of Psychiatry, Jinnah Hospital, Lahore
This case illustrates the psychological management of Delusional Disorder with Cognitive Behavioral Therapy. Assessment was done informally through Clinical Interview, Dysfunctional Thought Record, Subjective Rating of the Symptoms, Mental State Examination, and formally through the Brown Assessment of Beliefs Scale (BABS). Client scored 20 on BABS (2 points higher than its cut-off score of 18) which showed significant presence of Delusional Disorder. According to DSM-5 (considering client’s symptoms, results of her psychological assessment, duration of her illness and her daily life functioning), M.F. was diagnosed with 297.1 (F22) “Delusional Disorder, Persecutory type with bizarre content”. Psychotherapeutic intervention was comprised of Cognitive Behavioral Therapy (psycho-education, relaxation exercises, cognitive re-structuring through A-B-C model, verbal challenging, evidence for and against, assertiveness training and stress management techniques) which resulted in marked improvement in client’s symptoms. Client reported 80% improvement in her delusional beliefs and it was also confirmed by the psychological assessment done at pre and post level of therapy. The score was 6 on BABS after her therapeutic intervention which falls in the category of no significant delusions.
Key Words: delusional disorder, persecutory delusions, bizarre content.
Psychotic disorders are defined by abnormalities in one or more of the following five domains: delusions, hallucinations, disorganized thinking (speech), grossly disorganized or abnormal motor behavior (including catatonia), and negative symptoms. Disorders that come under the umbrella of psychosis are Delusional Disorder, Brief Psychotic Disorder, Schizophreniform Disorder, Schizophrenia and Schizoaffective Disorder (American Psychological Association, 2013).
Delusional Disorder is a rare type of psychosis in which a person presents with one or more delusions. People with Delusional Disorder may not exhibit hallucinations, disorganized behavior or mood incongruence. The marked feature of Delusional Disorder is that a person with this disorder continues to socialize and function in a normal way (Freeman & Garety, 2014). Clients with Delusional Disorder remain coherent, sensible and reasonable (Freeman & Garety, 2014).
Delusions with which a person having Delusional Disorder presents are fixed beliefs based on incorrect inference about external reality that persist despite the evidence to the contrary; these beliefs are not ordinarily accepted by other members of the person's culture or subculture. Delusions can be characterized as persecutory, referential, grandiose, erotomanic, grandiose, nihilistic or somatic (Leahy, 2003). Delusions can be bizarre or non-bizarre depending upon its contact with real life. The difference between a delusion and a strongly held idea is sometimes hard to make and depends in part on the degree of conviction with which the belief is held despite clear or reasonable contradictory evidence regarding its veracity (APA, 2013).
According to DSM-5, a person can be diagnosed with Delusional Disorder when there is presence of one (or more) delusions with duration of one month or longer and apart from the impact of the delusions or its ramifications, functioning is not markedly impaired and the behavior is not obviously bizarre or odd (APA, 2013).
The objective of the study was to check the efficacy of Cognitive Behavior Therapy for the treatment of Delusional Disorder.
Cognitive Behavior Therapy will significantly reduce client’s presenting complaints such as persecutory delusions.
Research Design
An ABA research design was used in the study to check the efficacy of CBT for the treatment of Delusional Disorder.
A single case was studied in this research method. Ms. M.F was a 26 years old unmarried woman and a general physician by profession. She had completed her studies in medicine from a government college and worked in anesthesia department of a private hospital. She had 3 older brothers and her birth order was last.
The client was in usual state of health four months back in November, 2018, when she got involved with one of her colleagues in her house job. They used to chat on text messages and when the client asked him to send marriage proposal to her house, he refused by saying that he was never involved romantically with her. Client started sex chatting on online websites after this rejection with unknown boys. And when she was not online, she started satisfying herself by touching and rubbing her private parts in frustration. One day while satisfying herself, she started noticing that she has an extra part on her vagina which nobody else has. She immediately went to washroom to check and noticed that she has two openings for urine instead.
Her online sexting continued till her brother got married with whom she used to share everything. She started forcing her parents to get her married too, her family accepted a proposal and she got engaged. Her engagement broke on some family issue and she was really disheartened after that incident. Client started doing a job to get herself busy and she reported to have her sexual urges in control on duty. One of her senior colleagues Dr. XYZ was un-married too and she often talked about the disadvantages of marriage. Client didn’t like her much. On the occasion of Eid once, her head of department called her in his office to give her Eid gift. He gave her blessings and kissed on her forehead. Client came home and remained tensed for rest of the day. She started searching on internet about the punishment on adultery. While reading about the quotations on adultery, she started saying that it was inserted in her mind by Dr. XYZ.
After that incident, she started saying that Dr. XYZ is conspiring against her and putting all these thoughts in her mind. She reported that Dr. XYZ has put cameras and she is keeping eye on everything. She refused to sleep alone afterwards, as she was scared that she’ll get punished. She reported having high sexual urges again. She forced her parents to get her married, but rejected the boy saying that he has one leg when her parents found her a suitable proposal. She kept forcing her parents to punish her on attempting adultery as she wasn’t innocent anymore. One day, she reported that she had green discharge and this thought is also inserted by Dr. XYZ. Her family members used to tell her a lot about the realities of these scenarios but the client always refused to understand and insisted on her beliefs.
Assessment was done informally through Clinical Interview, Dysfunctional Thought Record, Subjective Rating of the Symptoms, Mental State Examination, and formally through the Brown Assessment of Beliefs Scale (BABS).
Dysfunctional Thought Record (Wells, 1997). The purpose of the DTR was to increase client’s discrimination between the types of her thoughts. The cognitive distortions revealed from Dysfunctional Thought Record were Mental Filter, Overestimating Risk and Danger, what if thinking, Jumping to Conclusions, Personalization and Over importance of thoughts.
Table 1
Average Frequency and Intensity of the Thoughts Reported by the Client
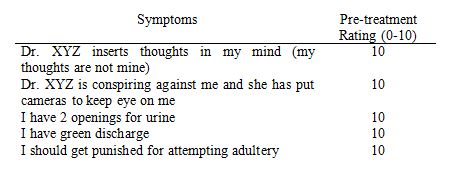
Subjective Ratings of the Symptoms by Client (Sommers- Flanagan, 2009). Subjective rating of the beliefs was taken from the client.
Table 2
Pre-treatment Subjective Rating of Symptoms by Client on 10-Point Rating Scale
Brown Assessment of Beliefs Scale (Eisen et al. 2001). Brown Assessment Belief Scale was applied to assess the client’s condition. Client scored 20 on BABS (2 points higher than its cut-off score of 18) which showed significant presence of Delusional Disorder.
Table 3
Pre-Treatment Scores of Client on Brown Assessment of Beliefs Scale
|
Raw Scores |
Cut-off Scores |
Category |
|
20 |
18 |
Significant |
The diagnosis of the client (considering client’s symptoms, results of her psychological assessment, duration of her illness and her daily life functioning), according to DSM-5 would be 297.1 (F22) “Delusional Disorder, Persecutory type with bizarre content”.
Case Conceptualization. The case was conceptualized on the model of Freeman and Garety (2014)
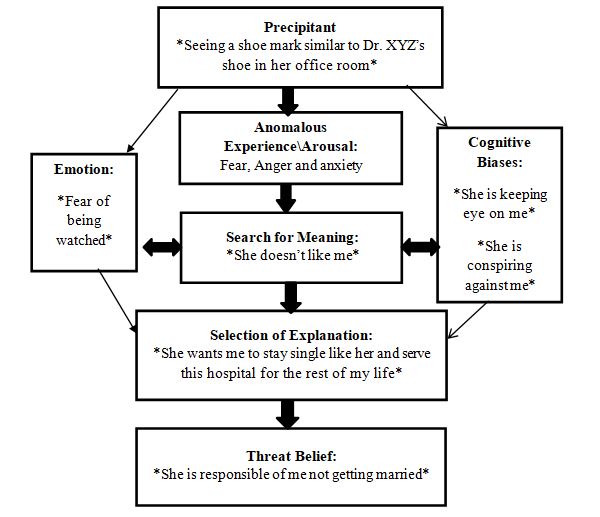
Figure 1. Case Conceptualization of Delusional Disorder Freeman and Garety (2014)
Cognitive Behavior Therapy was used to treat the client based on the etiological explanation and symptoms of the client.
This is client’s first psychiatric treatment and psychiatrists prescribed her antipsychotics olanzapine (2.5mg) and risperidone (2mg). Rapport was built with the client by giving her unconditional positive regard and she was psycho-educated about her symptoms through normalization (Donker, 2009). Progressive muscle relaxation, deep breathing and positive imagery were used to reduce her stress and anxiety (Jacobson, 1938). Verbal challenging was used to challenge her delusional beliefs such as thought insertions, odd beliefs (two openings for urine, green discharge), her constant need of getting punished and the fear of getting harmed by her colleague (Leahy, 1996). Evidence for and against was used to shatter the conviction of her delusional beliefs. Cognitive re-structuring techniques were also used to challenge and re-structure her delusional beliefs which were: thought insertions, odd beliefs (two openings for urine, green discharge) and the fear of getting harmed by her colleague (Leahy, 1996). Stress management techniques were used to teach her to cope with the future stressors of her life (Leahy, 1996; Wells, 1997). Social skills training, assertiveness training and problem-solving techniques were used to enhance her abilities to solve her problems and convey her message to others in a more effective way (Leahy, 1996). Therapy blue print was given to the client to prevent relapse (Leahy, 1996; Wells, 1997).
The summary of the 15 sessions conducted with the client is as follow:
In the first session, in order to develop compatible therapeutic relationship of trust with the client, she was actively listened. She was allowed to discuss her problems in detail. The client was given empathetic response towards her problems. A detailed clinical interview was conducted with the client to know the presenting complaints, history of the client’s illness, information about the family background, client’s personal history and premorbid personality.
In the second session, family and personal history were completed in order to know the precipitating and maintaining factors. The client was empathetically listened and given unconditional positive regard so that she could comfortably discuss her problems. For assessing the current functioning of the client, Mental Status Examination (MSE) and behavioral observation was done. Subjective ratings were collected from the client according to her current symptoms.
In the third session, the Brown Assessment of Beliefs Scale (BABS) was administered and questions related to other disorders were asked in order to rule out other problems for differential diagnosis. The prevalence rate of the disorder was explained to the client through normalization. She was also psycho-educated according to her disorder. At the end, she was taught deep breathing to relax.
In the fourth session, client was taught Progressive Muscle Relaxation technique to relax her body muscles and reduce her anxiety. Client felt really relaxed after completing the exercise.
In the fifth session, she was given a list of activities that she liked. She had to perform different tasks in her daily routine based on personal hygiene, her hobbies and social skills training.
In the sixth session, client was asked to rate her delusional beliefs on a scale of 0-100. She had to mark the number according to her belief on that specific delusion. In the initial sessions, she marked her delusions as 100 percent on the delusional belief scale.
In the seventh session, client was asked about her delusional beliefs and her thought insertions. When she explained all the scenarios, she was asked to provide evidence about those beliefs. When she couldn’t provide any evidence, she started to think otherwise.
In the eighth session, homework from the last session was checked. Client couldn’t provide any evidence on her beliefs. Client was briefed about the A-B-C model of Cognitive Behavior Therapy. She was explained about the purpose and procedure of A-B-C model.
In the ninth session, homework from the last session was checked. Client understood the concept of A-B-C model quite well. Client was again explained about the importance of her beliefs and the connection between belief and consequence of a scenario.
In the tenth session, homework from the last session was checked. Client seemed to understand the concept and provided right examples according to it. She was further explained about cognitive restructuring. And in the rest of the session, therapist and client discussed about re-structuring the beliefs and changing the consequences.
In the eleventh session, client seemed a little occupied and tensed. She was not responding to the planned activities. So, therapist had to change her session plan. Client was asked to talk freely about anything she wanted. She talked about her parents and her head of department. After that, she discussed about her father beating his wife and daughter.
In the twelfth session, client was taught to cope with the stress in a more suitable way. She was asked to take deep breaths and think about stressful situation in a logical way. Client was encouraged to exercise, meditate or walk whenever she feels herself in a bad mood. Client was encouraged to solve her future problems on her own. She was taught to make a list of possible solutions and then pick a preferred solution from that list and act on it.
In the thirteenth session, client was informed that the real purpose of assertiveness training is to increase the ability to straight forwardly express her feelings without getting passive. Client was explained about the three styles of communication: passive, assertive and aggressive. She was also taught to use assertive style of communication to explain her feelings to other person.
In the fourteenth session, client was asked to rate her symptoms according to her current functioning and post-treatment assessment was done. In the last session, client revised all the techniques carried out in the previous sessions in the form of therapy blue print that was provided to the client to help her deal with her condition if the symptoms slightly reappear again. Follow up sessions were also scheduled.
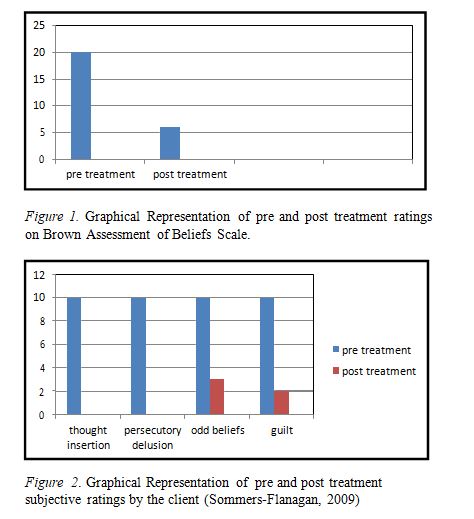
Post treatment assessment of client after 15 sessions showed marked decrease in her delusions (thought insertions, persecutory delusions). It indicated that there is a significant degree of effectiveness of Cognitive Behavior Therapy based therapeutic techniques for Delusional Disorder. Client’s odd beliefs and excessive fear were also decreased. When she couldn’t provide any evidence in favor of her delusions, she began to understand the goal of her therapeutic interventions. By understanding the A-B-C model thoroughly, she managed to provide scenarios against her delusions. The conviction of client’s belief upon her delusions was shattered through verbal challenging. Client reported to have 80% improvement in her delusional beliefs in her follow up session.
Freeman and Garety (2014) conducted a study on advances in understanding and treating persecutory delusions. According to their findings, six main factors mainly cause delusional thinking in a person, a worry thinking style, negative beliefs about self, interpersonal sensitivity, sleep disturbance, anomalous internal experiences and reasoning biases. These factors can be influenced by any social stressors or drug abuse in family (Freeman & Garety, 2014). Client had social and personal sensitivity which triggered her delusional beliefs and her alcoholic father also played a role in precipitating her illness. According to the above-mentioned factors, client had a worrying style of thinking, she also had negative beliefs about herself and she went through a trauma when her colleague rejected her. These factors led to the development of Delusional Disorder.
Freeman et al. (2016) conducted a research and the purpose of the research was to build a new psychological treatment which results in the full recovery of persistent persecutory delusions. The cognitive model treatment was applied to 11 patients in an average of 20 sessions. 7 out of 11 (64%) patients reported decrease in their persistent delusions which was supported by their post treatment ratings (Freeman et al., 2016). As client also reported decrease in her delusional beliefs, this shows the efficacy of cognitive behavioral intervention in treating delusions.
Limitations of the Study
As client’s mother was ill and couldn’t come to hospital so her personal history couldn’t be taken. Social Management couldn’t be done as social worker wasn’t available. As her mother wasn’t available so Family Counseling couldn’t be done properly.
References
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Washington, DC: Author.
Beck, J. S. (1995). Cognitive therapy: Basics and beyond. The Guilford Press.
Davis, M., Eshelman, E. R., & McKay, M. (1982). Relaxation and stress reduction workbook. Oakland: New Harbinger Publications.
Ellis, A., & MacLaren, (1998). Rational emotive behavior therapy, A therapist’s guide. USA: Impact Publishers.
Freeman, A., Pretzer, J., Fleming, B., & Simon, K. M. (2004). Clinical applications of cognitive therapy (2nd ed.). New York, NY: Kluwer Academic/Plenum Publishers.
Freeman, D., Bradley, J., Waite, F., Sheaves, B., DeWeever, N., Bourke, E., McInerney, J., Evans, N., Černis, E., Lister, R. and Garety, P., 2016. & Garety, P. (2016). Targeting recovery in persistent persecutory delusions: a proof of principle study of a new translational psychological treatment (the Feeling Safe Programme). Behavioural and Cognitive Psychotherapy, 44(5), 539-552. doi: 10.1017/S1352465816000060
Freeman, D., & Garety, P. (2014). Advances in understanding and treating persecutory delusions: a review. Social Psychiatry and Psychiatric Epidemiology, 49(8), 1179-1189. doi: 10.1007/s00
127-014-0928-7
Eisen, J. L., Phillips, K. A., Beer, D., Atala, K. D., Rasmussen, S. A. & Baer, L. (2001). Brown Assessment of Beliefs Scale. Retrieved from http://www.veale.co.uk/wp-content/uploads/2010/11/BA BS_revised_501.pdf
Kring, A. M., Johanson, S. L., Davison, G. C., & Neale, J. M. (2010).
Abnormal psychology (11th ed.). USA: John Willy sons.
Leahy, R. (2003). Cognitive therapy techniques: A practitioner’s guide. USA: The Guilford Press.
Miltenberger, R. G. (1997). Behavior modification: Principles and procedures. Belmont, CA: Wadsworth.
Sommers-Flanagan, J., Sommers-Flanagan, R. (2009). Clinical Interviewing. USA: John Wiley & Sons, Inc.
Spiegler, M. D., & Guevremont, D. C. (1959). Contemporary behavior therapy. USA: Brooks/Cole Publishing Company.
Wright, J. H., Basco, M. R., & Thase, M. E. (2006). Learning cognitive-behavior therapy: An illustrated guide. USA: American Psychiatric Publishing, Inc.