*Khola Tahir
Centre for Clinical Psychology, University of the Punjab, Lahore, Pakistan
Clinical Psychologist, Sir Ganga Ram Hospital, Lahore
Mr. X, was 28 years old. The patient came with complaints of excessive worry and not being able to control it, apprehensiveness that his mind would go blank and that he would lose his mind if kept worrying, fear of being inadequate at work, unable to concentrate on work, anxiety and tiredness. He also reported disturbed sleep and muscle tension. He was diagnosed as having Generalized Anxiety Disorder and his case was conceptualized using the Well’s Cognitive Model of Generalized Anxiety Disorder. Management was also done on the CBT model. Treatment goals were achieved by the use of various verbal challenging exercises such as questioning the evidence, evidence for and against, challenging uncontrollability appraisals and by providing education in order to normalize the worry. Various behavioral exercises such as controlled worry periods, challenging uncontrollability beliefs, loss of control experiments, pushing worry limits in situ and abandoning thought control were also done for disconfirming the beliefs related to Type II worry. The patient showed significant improvement in his condition by the termination of the therapy which was evident through his post assessment ratings.
Key Words:generalized anxiety disorder; cognitive behavior therapy; verbal challenging; behavioral experiments
Among other anxiety disorders such as Panic Disorder, Obsessive Compulsive Disorder etc, Generalized Anxiety Disorder is also very common among adults. It has been estimated that up to 20% of adults suffer from either one form of anxiety in their lives (Munir & Takov, 2019). Generalized Anxiety Disorder (GAD) is characterized by persistent, excessive and unrealistic worry about different matters ranging from personal life, academic or occupational life. The worry is excessive and difficult to control and leads to many psychological and physical symptoms (American Psychiatric Association, 2015).
Apart from excessive worry, Diagnostic Statistical Manual for Mental Disorders (DSM-5) has also stated that this excessive worry is difficult to control and should have at least three or more physiological and cognitive symptoms such as restlessness, easily fatigued, difficulty concentrating, muscle tension, sleep disturbance, and irritability (American Psychiatric Association, 2015). Stress in one’s life, physical conditions such as diabetes or stress, genetic factors, environmental factors such as child abuse and substance dependency are all important etiological factors of GAD (Munir & Takov, 2019).
Cognitive Behavior Therapy is one of the most effective way of treating various disorders such as depression and anxiety. It has been indicated that CBT and its exposure based modalities are effective to treat anxiety disorders such as GAD (Olatunji, Cisler, & Deacon, 2010). Cognitive Behavior Therapy includes techniques like verbal challenging for cognitive restructuring and behavior experiments. In addition, relaxation exercises are also used to treat symptoms like fatigue and tiredness (Otte, 2011).
During the initial sessions, psycho-education was done to develop an insight about the disorder as well as the etiological and maintaining factors. Further, verbal challenging exercises were done which mainly include techniques like questioning the evidence, cost benefit analysis, questioning the mechanism, selling the meta-worry and challenging uncontrolled appraisals. Whereas, behavioral experiments include suppression experiments, controlled worry periods, loss of control worry experiments, and pushing worry limits in situ (Wells, 1997).
Various studies have established the effectiveness of CBT for various anxiety disorders such as GAD. However, it has been suggested that the techniques of CBT are specific for each disorder (as cited in Otte, 2011). Therefore, the purpose of this study is to examine the effectiveness of CBT in treating GAD, which would help the future clinicians and practitioners to treat such disorders by modifying the therapeutic techniques according to client needs.
The objective of the study was to check the efficacy of Cognitive Behavior Therapy for treating Generalized Anxiety Disorder.
Cognitive Behavior Therapy will significantly reduce patient’s presenting complaints such as excessive worry about his performance at work, anxiety related to not be able to read properly if said so, and apprehensiveness of his mind going blank due to worrisome thoughts. Furthermore, CBT will reduce disturbed sleep patterns, fatigue, difficulty concentrating at work, and irritability.
Research Design
An ABA research design was used in the study to check the efficacy of CBT in treating GAD. In this research design assessment is done prior to the treatment and after the treatment is given.
The sample consisted of a 28 years old man who had done bachelors in Commerce and was the second last born among five siblings.
In 2009, the patient’s problems became evident after his father’s death. The patient felt extremely distressed as he was much close to his father. The patient reported that after few days of his father’s death, he remained worried. He was uneducated and jobless which made him worry about him and his family’s future. Mr. X, was unable to control the worry and he felt that if he wouldn’t stopped worrying, he would lose his mind. This caused a decrease in his sleep and he started experiencing muscle tension especially pain in his shoulders. Mr. X, reported that while worrying he would make plans how to stop himself from worrying. In order to overcome his worries, he tried finding new jobs but was unable to find any reasonable job because of lack of adequate education. The patient reported that it was because of his worrisome thoughts, he decided to study for which he took admission in a government college in I.Com.
While Mr. X was preparing for his exams he was worried that he would not be able to perform in exams and his mind would go blank after seeing the paper. He reported that he became extremely worried that these thoughts would make him go crazy and would affect his performance. He also felt that his mother would be utterly disappointed. The patient felt that these thoughts were overwhelming for him and he found it extremely difficult to control them. He remained worried about the future and that he wouldn’t be able to get a reasonable job. He felt that he would lose his mind if he continued studying. These thoughts led him to leave his studies and he got appointed as a peon at a private firm in the latter part of the year 2009. The patient felt that the job however, was below his status but he was happy with it as he had to write and read nothing and was only there to do sweeping and some cleanliness tasks. He felt that during this job, no one would ask him whether he could read or write. During his job, he sometimes became worried and anxious regarding his performance. He had worried thoughts that the money would not be enough and he would be left behind his peers.
In the year 2012, the manager who he befriended and knew that Mr. X had some educational background offered him the job of cooperate coordinator. The patient was elated and he took the job. At first, he faced no difficulty. After a year in 2013, the patient used to become anxious whenever assigned the new task and this led him to worry about the outcome. He became worried of his own performance and what if he was unable to deliver what was demanded of him. He had thoughts related to people knowing that he knew nothing which was a cause of great distress for him. He reported that he knew most of the work he did there still he felt great distress regarding the job. He often had thoughts as to why was he worrying when he knew everything. These thoughts were so overwhelming for him that he decided to quit his job in 2014.
While Mr. X was jobless, in 2015, his mother kept talking to him about getting married. The patient reported that for no apparent reason, he started worrying that he had no job and his marriage would fail thus, in order to prevent that from happening he should be able to find a job with reasonable salary. The patient reported, though he was not getting married any time soon still it got him stressed out thinking about it. The patient thought that his worrying was uncontrollable and was making him crazy.
After 3 months of him looking for the job in December 2015, the patient got a job at an AC repairing workshop. At the present job, the patient worried that his boss was not satisfied with his job and he would be jobless very soon which would cause problems for his family. The patient consulted a general physician who advised him to see a psychotherapist to deal with his problem. Mr. X, came with the complaints that he was constantly worried about the future for no apparent reason. He felt that the worrying was uncontrollable and was controlling his mind. He also worried that he would end up losing control and if he wouldn’t stop worrying and he would go crazy. This pattern of worrying made the patient to concentrate less on work and restless. He also reported disturbed sleep patterns as he was unable to sleep properly.
Patient’s family had no history of any psychiatric history. Written consent was taken from the patient in order to ensure his willing participation. He was further ensured of confidentiality and informed that he can withdraw anytime he wanted.
Generalized Anxiety Disorder Scale (GADS) (Wells, 1995). Generalized Anxiety Disorder Scale was administered in order to find out the severity of the problem and to evaluate therapy outcome. It also revealed the patient’s coping strategies in order to deal with the worry and the avoidance behaviors associated with it. The profile of the patient revealed that he often tried to control the worry but it was below the moderate level. The profile also gives an indication that the patient often displayed the efforts in order to cope with the worry by distracting him, looking for evidence, and planning to cope with the worries if they would come true. He also became cautious and tried to control his worry. See table 1 for pre and post assessment.
Anxious Thought Inventory (AnTI) (Wells, 1995). The scores on the first scale of AnTI, Social was 32 and the patient scored high on items like he felt he was a failure, he was unable to live up to expectations of the people and thoughts as if he would do something wrong. The patient had also been worried with thoughts of being a failure, inability to cope like others, and worry of making a fool of himself. The score on the second subscale was 20 which indicates that patient had also been worried about his health. Whereas, the patient got the score of 25 on the third scale Meta. The items on this scale indicate that patient often thought about his future negatively than positive, and find himself difficulty in clearing his mind. See table 2 for pre and post assessment.
On the basis of the formal and informal assessment, MR. X was given the diagnosis of 300.02 (F41.1) Generalized Anxiety Disorder according to DSM-5.
Case conceptualization. The present case was conceptualized on the meta-cognitive model of GAD (Wells, 1995). The model explains the cognitive factors which helps in the development and maintenance of the disorder. The model helps in distinguishing the type 1 worry from the type 2 worry. Type 1 is the basic type of everyday worry whereas type 2 worry is worry about worry. The patients with GAD negatively appraise the worry known as type 2 worries which are the beliefs held by the patient about worrying. These beliefs about worrying often produce negative effects in the form of emotions, behaviors and thought control. These three factors are often found to be involved in the escalation and maintenance of the problem.
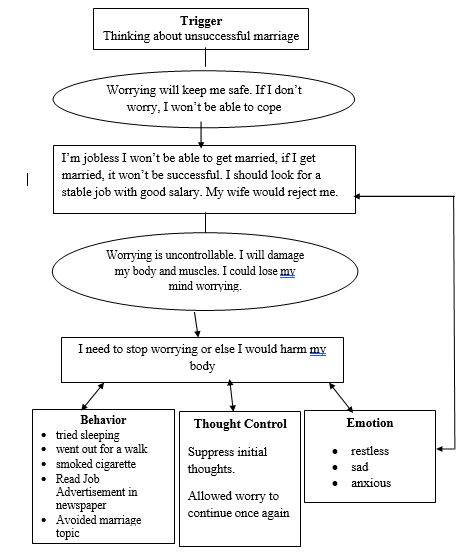
Figure1. Case Conceptualization on Meta-Cognitive Model of GAD
Session 1
Session 3
Session 5-6
Session 2
Session 4
Session 7-8
(normalizing worry)
Session 9-10
Session 11-12
After management of the patient’s complaints, post-assessment was done. The results of the post-assessment are provided in tables.
Table 1
Subjective Ratings of the GADS at the pre-treatment and post treatment level.
|
Areas |
Pre-assessment Ratings (8 point scale) |
Post-assessment Ratings (8 point scale) |
|
Distressing worries over the |
05 |
02 |
|
last week |
|
|
|
Effort to control the worry |
03 |
01 |
|
Tried to cope with worry |
06 |
01 |
|
Avoidance |
06 |
01 |
Table 2
AnTI scales and their total scores.
|
Scales |
Pre-assessment Scores |
Post-assessment Scores |
|
Social |
32 |
11 |
|
Health |
20 |
08 |
|
Meta |
25 |
09 |
|
Total |
77 |
28 |
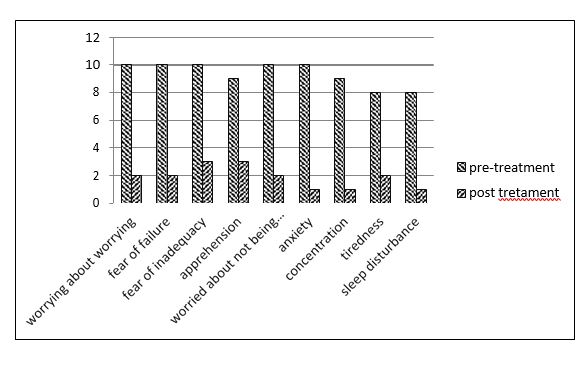
Table 3
Pre and Post treatment ratings on a 10-point rating scale as reported by the patient
|
Symptoms |
Pre-treatment Ratings |
Post-Treatment Ratings |
|
Excessive worry about being |
10 |
02 |
|
worried most of the time |
|
|
|
Fear of failure |
10 |
02 |
|
Fear of being inadequate at |
10 |
03 |
|
work |
|
|
|
Apprehensions about future |
09 |
03 |
|
Excessive worrisome thoughts |
10 |
02 |
|
that he won’t be able to read or |
|
|
|
write or perform |
|
|
|
Anxiety |
10 |
01 |
|
Lack of concentration |
09 |
01 |
|
Tiredness |
08 |
02 |
|
Sleep disturbance |
08 |
01 |
The patient in the present case displayed apprehension related to future, and the fear of performance in some of the settings such as job, worried about not being able to earn enough money and fear that he would lose control and would run away from the place. The patient often remained restless, slept more than the usual, feeling tensed, fatigued and pre occupied with the worrisome thoughts. The patient had also been found to be indulged in safety behaviors such as listening to songs and avoidance behaviors such as not showing up for work and not wanting to think about those thoughts. The following symptoms were consistent with the Generalized Anxiety Disorder diagnosis according to DSM-5. According to DSM-5 (APA, 2013) a person becoming excessively worried and apprehended most of the time for at least 6 months and not being able to control the worry despite trying would give an indication of the diagnosis of Generalized Anxiety Disorder. The patient should also experience three or more of the associated symptoms such as fatigue, feeling easily keyed up, sleep problems etc most of the day for the diagnosis of GAD. Moreover, the symptoms should be severe enough to cause significant impairment in social and occupational functioning of the patient. All these symptoms helped in formulating the diagnosis of the current patient.
Beck (1985) suggested that people with GAD are always uncertain and hold certain assumptions that (for example, “A situation or a person is unsafe until proven to be safe” or “It is always best to assume the worst”) that imply they are in imminent danger (as cited in Comer, 2012). This could be one assumption held by the patient thus helped in the development and maintenance of the patient’s disorder.
Salkovski’s (1991) proposed a cognitive model describing the relationships between the threat belief and safety seeking behavior. He proposes that for any individual safety seeking is linked with the perception of serious threat. This relationship between the two would most likely maintain the anxiety and panic attacks. In the current case the patient often used various avoidance behaviors like not going to the same route. This could be one of the probable explanations of why the patient has maintained the disorder.
Most of the behavioral experiments conducted were between sessions which could have affected the validity of the experiments if the experiments not conducted right. Moreover, self-report measures used in the study may be vulnerable to social desirability and demand characteristics that cannot allow the conclusion that independent observers would verify that actual anxiety was altered.
References
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Washington, DC: Author.
Comer, R. J. (2010). Abnormal Psychology. USA: Worth Publishers Davison, G. C. & Neal, J. M. (2001) Abnormal Psychology. New
York: John Wiley & Sons.
Munir, S. & Takov, V. (2019).Generalized Anxiety Disorder in Stat Pearls Treasure Island. StatPearl Punlishing. Retrieved from: https://www.ncbi.nlm.nih.gov/books/NBK441870/
Otte, C. (2011). Cognitive behavioral therapy in anxiety disorders: current state of the evidence. Dialogues in Clinical Neuroscience, 13(4), 413–421.
Olatunji, B. O., Cisler, J. M., & Deacon, B. J. (2010). Efficacy of cognitive behavioral therapy for anxiety disorders: a review of meta-analytic findings. The Psychiatric Clinics of North America, 33(3), 557-577. doi: 10.1016/j.psc.2010.04.002.
Wells, A. (1995). Meta-cognition and worry: A cognitive model of generalized anxiety disorder. Behavioural and Cognitive Psychotherapy, 23(3), 301–320.
Wells, A. (1997). Cognitive Therapy of Anxiety Disorders: A practice manual and conceptual guide. New York: John Wiley & Sons
Salkovski, D. M. (1991). The Importance of Behavior in the Maintenance of Anxiety and Panic: A Cognitive Account. Behavior Psychotherapy, 19(1), 6-19. doi: 10/1017/S014134730
001472