Quality of Life, Self Esteem, Coping, Rejection Sensitivity and Depression among Infertile Men and Women
Rabia Usman
Applied Psychology Department, Kinnaird College for Women, Lahore, Pakistan
*Masha Asad Khan
Applied Psychology Department, Kinnaird College for Women, Lahore, Pakistan
This study investigated quality of life, self-esteem, coping, rejection sensitivity and depression among infertile men and women of Lahore. Through purposive sampling data was collected from two private hospitals of Lahore from 120 infertile individuals, with female age ranging between 22-45 years (M=30.91; SD= 5.26) and male age ranging between 24-53 years (Mage=35.1; S. D=6.97). Correlation research design was used. Ferti Quality of Life Scale, Rosenberg Self Esteem Scale, Coping Inventory for Stressful Situations (CISS), The Adult Rejection Sensitivity Questionnaire (ARSQ), Beck Depression Inventory-II and Demographic Questionnaire were used for assessment. Results of Pearson Product Moment Corelation showed a significant positive relationship in quality of life, self-esteem,avoidance coping and problem focused coping among infertile individuals. A significant negative relation was found in the quality of life,depression and emotion focused coping. A significant correlation in the quality of life with depression, self-esteem and emotion focused coping and a non- significant correlation exist among individuals in the quality of life with rejection sensitivity, avoidance coping and problem focused coping was found. The regression analyses results predicted that depression, self- esteem and emotion focused coping to be strong predictors of quality of life in infertile individuals.
Keywords: infertility, depression, self-esteem, quality of life, rejection sensitivity, coping
The present study examined the relationship of quality of life, self-esteem, coping, rejection sensitivity and depression among infertile male and female individuals from Lahore.
According to Fisher and Hammarberg (2017), infertility is the psychological and emotional changes experienced by a couple who gets diagnosis of infertility. Infertility has the potentiality of affecting couples who have certain feelings such as humiliation, mistrust, social withdrawal and anger (Datta, et al, 2016; Tulppala, 2002). Infertility has been perceived as a taboo and a sensitive topic to engage in. About 75% of the infertile couples feel that they are given appropriate support from the family or their close friends. Due to the nature of the topic of infertility, many couples keep the topic as secret even when attending clinics (Salzer, 1994). According to Marcia &Patrizio (2015) on his way of finding out infertility issues, claimed that approximately 186 million people are affected with infertility around the globe. On the other hand infertility ratio in Pakistan is 1:5 in married couples (Ali et al., 2011)
According to Cavdar and Coskun (2018) self-esteem indicates the extent to which an individual trust one’s self for certain skills, worthiness and success. Drawing from this proposition, infertile individuals viewthemselves as dysfunctional, an attribute that may deteriorate their self-image and self-esteem (Miall, 1994).Tiitinen (2009) hypothesized that diagnosis of infertility also has psychological trigger which may lead to a sequence of deep emotional annoyance and insecurity accompanied by depression or anger. The mental trigger generates a feeling of hopelessness, guilt, depression, helplessness, defeat and mourning. Therefore, infertility leads to low self-esteem eventually leading to poor quality of life.
Dural et al. (2016) on the other hand define quality of life as a combination of love, happiness, joy, self-esteem and peace. Infertility impacts a person’s quality of life and so does its management. In an effort to mitigate stress, infertile individuals use a number of coping mechanisms.
Various studies have focused on assessing the relationship between infertility and coping emotional distress. Coping mechanisms are imperative in averting distress related to infertility (Jahromi & Ramezanll, 2015) On the other hand, Stewart, Pasternak, Pereira and Rosenwaks (2019) noted that infertility is a unexpected event. Besides, men apply more separating and controlling approaches as compared to women. Jennifer, Marci, Silvina, James, and Lisa (2017) conducted a study to examine the physiological and emotional concomitants of diagnosis of infertility in women. The study indicated that women who had primary infertility as a result of diminished ovary were more likely to experience depression and stress. They suggested that distress surrounding infertility has a significant association with the manner in which women responded to learning. From this viewpoint, coping strategies were seen to be associated significantly and positively with an individual’s quality of life.
According to Carranza-Maman et al., (2015) individuals who are not aware of infertility related issues or did not seek any kind of help or are usually shy to ask their family or friends, is an attribute that leads to lower social support. Due to lack of awareness, individuals in a community may make senseless comments about their childlessness. This high level of distress increases even more when an individual feels lonely or feels there is low social support that culminates to a poor relationship with the infertile individual. Pasch and Sullivan (2017) argued that women from an infertile family attempt to absorb a significant proportion of husband’s blame for infertility, this way women provide a support to their husband infertility related problems. In addition, men also become resistant to accompany their wives to infertility clinical setting and give excuses such as loss of time, increased expenditure, foregone opportunity cost in relation to income among others. Hence infertility may be linked with low quality of life in men and women.
Accrding to Tiitinen (2009), depression as a result of infertility significantly affects the quality of life of idividuals. He argued that infertility is caused by different reasons such as tubal issues (10-15%), breakdown of ovulatory system (20-30%), poor quality of sperms (10- 15%) and endometriosis (10-20%). Winkelman et al., (2016) indicated that age of women is the most critical aspect regarding infertility as 25 years and above fertility reduces as age progresses. Chou (2004) indicated that infertile females experience high mental distress than ordinary partners. The occurrence of depression among infertile couples under infertility treatment is altogether higher with approximate assessments of real depression in the range of 15-54% (Chou, 2004).
Rejection sensitivity on the other hand is restlessness of an individual as a result of failed expectations of recognition and acceptance from certain others. In essence, the situation occurs when an individual receives strong negative rejections. This approach predisposes such an individual to situation of being hyper vigilant that is related to aggressiveness and anxiety. According to Alosaimi, Altuwirqi, and Bukhari (2015), individuals with high rejection sensitivity are more likely to be displeased with personal relationships or becoming displeased with any signs of romance. This eventually leads to low self-esteem among such individuals, an aspect which negates with their overall quality of life. Ibrahim, Brackett and Lynne (2016) reported thoughts of rejection trigger negative attitude among individuals therefore culminating into poor quality of life. While rejection due to infertility may be linked to depression, it also has the ability to culminate into poor overall health.
RationaleAVarious stressors associated with infertility including stress related to sexual functioning, fortitude, variety of affiliationand changes in family and social network has been reported by couples (Newton, Sherrard, & Glavac, 1999). In an effort to manage stress, infertile individuals use number of coping mechanisms. Various studies focused on the relationship of infertility with coping, emotional distress.Coping mechanisms have been linked to reduction of infertility related distress and stress (Tennen, Affleck, & Mendola, 1991). Infertile people may cope up with their loss by collapsing into depression and which may be health related, anxiety, distress and grief (Berghuis & Stanton, 2002; Van Den Akker, 2005). The findings of the present study provide basis for clinicians to design and develop educational and interventional programme for infertile individuals with a major focus on reducing depression, rejection sensitivity and elevation self-esteem and quality of life. Further, with a focus on adapting effective coping styles. Studying these variables can help clinical psychologists to improve quality of life through making effective and practical interventions and mental health of infertile individuals.
Objectives of the Study- To check relationship of quality of life, self-esteem, coping, rejection sensitivity and depression among infertile men and women.
- There is a significant relationship in quality of life and self- esteem among infertile individuals.
- There is a significant relationship in quality of life and the Coping styles ie. Avoidance coping, problem focused coping, emotion focused coping among infertile individuals.
- There is a significant relationship in quality of life and rejection sensitivity among infertile individuals.
- There is a significant relationship in quality of life and depression among infertile individuals.
Method
Research Design
Correlation research design was used to check relationship of the variables in the target population. This research design was implemented to investigate the relationship among two or more variable. Whole purpose of using correlations in research is to figure out which variables are connected (Miller,2003).
SampleThrough purposive sampling data was collected from 120 infertile individuals (females=68; males=52). The age range of infertile females was between 22 to 45 years (M= 30.01; SD 5.26) and the age range of males was between 24 to 53 years (M=35.1; SD 6.97). The data was collected from November 2014 to February 2015, it included participants from two infertility clinics/hospitals of Lahore. The inclusion criterion for selection of sample was being married and diagnosed with infertility with at least one year of their marriage.
Assessment MeasuresThe Demographic Questionnaire. A self-constructed demographic form was used to collect personal information from the participants, which include; age, education, years of marriage, years of infertility, reasons of infertility and family infertility. The participants had different educational level from matric (31.67%), F.A (26.67%), Bachelors (20%), masters (23.33%) to PhD. (0.83%). The infertility is also affected by age, family marriages (32.5%), infertile couple within the family (32.5%) and various reasons of infertility i.e. Polycystic (21.67%), age factor (4.17%), recurrent abortions (10.83%), general medical condition (10%), oligospermia (21.67%), asthenospermia (15.83%), tubal blockage (3.33%) and others (7.5%).
FertiQuality of Life Scale (Boivin, Takefman & Braver man, 2008). Ferti quality of life scale,a 36 item scale with 5-point likert scale, will be used to assess the quality of life among infertile couples. The questionnaire is divided into 4 domains including overall, personal, interpersonal and healthcare. Moreover, it has 9 dimensions i.e., emotional, psychological, physical, values, partner relationship, and social network, occupational, medical and psycho educational. Higher scores indicate higher quality of life. The test retest has been reported ranging from 0.71 to 0.94.
Rosenberg Self Esteem Scale (Rosenberg, 1965). The Rosenberg Self-Esteem Scale is a 10-item scale using a 4-point Likert scale ranging from ‘strongly agree’ to ‘strongly disagree’. Scores falling between 15 and 25 indicate normal range. The higher score shows higher self-esteem and vice versa. Internal consistency ranges from 0.77 to 0.88.
Coping Inventory for Stressful Situation (Endler & Parker, 1999). The coping inventory for stressful situation is 21 item self-report questionnaire All items were answered on 5 point Likert scale ranges from ‘0’ “not at all to ‘5’ “very much”. The test retest reliability has been reported as 0.85 and validity is 0.90.
Adult Rejection Sensitivity Questionnaire (A-RSQ) (Berenson, Downey, Rafaeli, Coifman & Paquin, 2011). The Rejection Sensitivity Questionnaire (RSQ) has 18 questions that seek to show the levels of interpersonal interactions. The ARSQ consists of nine hypothetical situations involving interactions with partners, family, friends, and strangers, with potential rejection. It consists of nine situations involving interactions with partners, family, friends, and strangers, with potential rejection. Respondents rate the degree of their concern or anxirty over their reaction and the expectancy to be rejected on a 6-point Likert-type scale ranging from 1, “very unconcerned” to 6, “very concerned” and from 1, “very unlikely” to 6, “very likely”. The alpha reliability coefficient is 0.89.
Beck’s Depression Inventory (BDI)-II (Beck, Rush, Shaw, & Emery, 1979). Beck Depression Inventory consists of 21 items. It is rated on a 4 point likert scale ranging from 0 to 3. The BDI score was obtained by adding all the numbers marked suitable by the participant of all 21 items. The total score of depression on the scale range from ‘0’ to ‘63’ and normally divided into four categories. Lower scores ranging from 0 to 9 indicates normal whereas high score ranging from 24 to 63 indicates extremely severe depression. The higher the score the higher will be the depression. The questionnaire takes 5 to 10 minutes to complete. The Cronbach’s alpha for BDI was 0.70.
ProcedureWritten permission was obtained from the administration of respective hospitals and from the participants of study. They were briefed about the study. Furthermore, the participants were assured about confidentiality of data and that these would solely be used for the research purpose. The participants were informed about their right to withdraw from the study at any point in time. The participants were administered the measures of study individually, these included: Quality of life; Rosenberg Self Esteem Scale; Coping Inventory for Stressful Situation; Adult Rejection Sensitivity Questionnaire and Beck’s Depression Inventory-II, respectively. Individual testing was conducted. The total administration time was 40-45 minutes approximately.
Results
Table 1 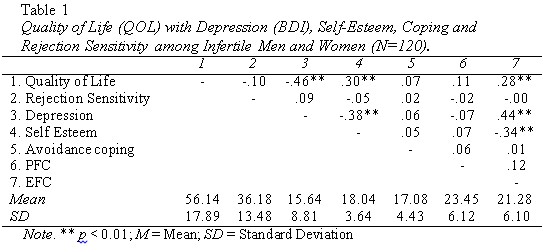
Table 1 shows positive correlation between quality of life and avoidance coping and negative relationship between quality of life and emotion focused coping among infertile men and women. However, non-significant relationship was found in quality of life and rejection sensitivity in the sample.
Table 2 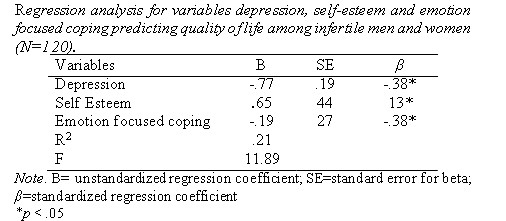
Table 2 shows a simple linear regression carried out to ascertain the extent to which depression, self-esteem and emotion focused coping can predict quality of life scores. The overall regression model predicted 21% of the variance. The regression analysis of highly significant values predicted that depression, self esteem and emotion focused coping strongly predict quality of life in the sample.
Discussion
The diagnosis of infertility may bring along a horde of changes in the life of the individuals which may be reflected in the quality of life, self-esteem, and coping styles of individuals along with more sensitivity to rejection and manifestation of depressive symptomatology among infertile people. Our findings showed that the quality of life increased with the increase in the self-esteem among infertile men and women. Anate and Wischmann (2014)conducted research to investigate the relationship between self-esteem and the quality of life in females with infertility but had received sociological support. The findings illustrated that self-esteem helped boost the morale of the person suffering from infertility hence enhancing his/her quality of life. Most people who have infertility issues usually find it challenging to interact with other people fearing that community would judge them for their misfortunes. Thus, poor socialization ability adversely affects their quality of life.
Our results demonstrated positive correlation between quality of life and avoidance coping among infertile individuals which indicates that as the avoidance coping increases the quality of life also increases. Schmidt, Holsten and Bovein (2005) found that men and women develop various avoidance coping skills to overcome the social and emotional challenges associated with infertility. There are various strategies that people use to overcome stressful events due to infertility including engaging in personal work instead of interacting with other people. Such strategies have been found to have a positive impact on their quality of life as they help the persons forget their issues.
The findings of present study divulged a positive relationship between quality of life and problem focused coping. Rashidi et al. (2011) in their research found that infertility stress abridged when couples facing fertility issues develop their own exclusive coping strategies. The existing literature and present study revealed a non- significant relationship between quality of life and problem focused coping despite the fact that the results of correlation showed a positive relation. Infertile individuals do not stride towards implementing problem focused coping because they may view the issue of infertility to be untreatable.
Inverse relation between emotions focused coping and quality of life findings are in line with the previous findings of Butler and Nolen- Hoeksema (1994) as they mentionedthat women use worry as a strategy to deal with anxiety, called emotion focused coping, which is more likely to continue as depression than active emotion focused coping techniques such as drugs usually used by men. According to Berghuis and Stanton (2002) when men and women go under treatment for infertility they experience more emotional challenges. Though couples face infertility together, their emotional reactions differ a lot and this difference shows that how they cope up this stressful situation. Since emotion focused coping focuses more on denial and distraction especially in infertile individual, females feel better when using emotion focused coping. A women's experience of infertility produces a feeling of shock, refusal, dissatisfaction, self-doubt, disappointment, anger guilt blame, and even depression, hampering a better quality of life for infertile couple.
Result showed non-significant relationship in quality of life and rejection sensitivity among infertile individuals. Whereas, Palomba et al. (2018) found that an increase in rejection sensitivity among infertile women led to the decrease in the quality of life.The findings obtained from the study were in contrast the findings from the current study. This difference may be explained as in the light of cultural context and operational definition of the variable as Palomba et al. (2018) defined the quality of life in terms of emotional stability and social well-being. However, it was evident that women suffering from infertility require emotional support and a feeling of acceptance from the community. Thus, if they feel that they are not accepted by their families, they may experience emotional instability which affects their quality of lives.
Significant relationship was found in quality of life and depression which shows that the quality of life increases with the decrease in depression among infertile individuals. Results have been supported by the research conducted on the relationship between quality of life and distress among infertile couples by Aarts et al. (2010). They reported that infertile couples with high scores on quality of life scale revealed lower levels of depression and anxiety whereas infertile couples who had low quality of life showed more somatic complaints and distress. Aliyeh and Laya (2007) also conducted a similar research on the quality of life and depression on infertile Iranian women. The study showed that women, unlike men, experience depression which adversely affects their ability to socialize or vice versa.
Implication for Future ResearchThe future implications of these findings can be that a mixed research design should be used in order to study the same variables in depth like rejection sensitivity and self-esteem along with coping styles. In order to decrease rejection sensitivity, depression, and increase self- esteem, quality of life and improve coping of infertile individuals, psycho-educational programsmay be introduced in the hospitals. A preventive programs can be designed by keeping in view the mental health of infertile individuals an intervention may be designed based on the principles of cognitive behavior therapies to help them cope with the situation of infertility.
Limitations and SuggestionsThe data was drawn using purposive sampling therefore findings of the study could not be generalized. Only bilingual and educated subjects participated in the study because the tools used in the study were available only in English language. This exposed the study to selection bias. Additionally, the study only included people living in Lahore metropolitan city who have cultures that may be different from people living in other places. Thus, the findings may not be generalized to cover people from regions with cultures that are different from the culture and practices within Lahore. Sample from other cities should also be taken and Cross sectional study could be administered. Longitudinal study could be done. Further, mixed method approach may also be an effective strategy.
References
Aarts, J. W., Empel, I.W., Boivin, J., Nelen, W. L., Kremer, J. A. &Verhaak, C. M. (2011). Relationship between quality of life and distress in infertility: A validation study of the Dutch FertiQoL. Human Reproduction,26, 1112–1118.
Aliyeh, G., & Laya, F. (2007). Quality of life and its correlates among a group of infertile Iranian women. Journal of Medical Science Monitory, 13, 313-317.
Anate, M., & Akeredolu, O. (1995).Surgical management of female infertility in Ilorin, Nigeria. East African Medical Journal, 72(7), 411- 414.
Berghuis, J. P., & Stanton, A. L. (2002). Adjustment to a dyadic stressor: A longitudinal study of coping and depressive symptoms in infertile couples over an insemination attempt. Journal of Consulting and Clinical Psychology, 70(2), 433-438.
Boivin, J., Takefman, J.,& Braverman, A. (2008).The fertility quality of life; development and genralpsycholometric properties. Fertility and Sterility, 96(2), 409-415.
Carranza-Maman, B., Havelock, J., Hemmings , R. C., Sierra, S., Case, A., & Vause , T. (2015).The management of uterine fibroids in women with otherwise unexplained infertility. Journal of Obstetrics and Gynaecology Canada, 37(3), 277-285.
Cavdar, N. K., & Coskun, A. M. (2018). The effect of infertility upon quality of life and self-esteem. MOJ Women’s Health, 7(3), 89- 94.
Chou, K. L. (2004). Childlessness and psychological well-being in Chinese older adults. International Journal of Geriatric Psychiatry, 19, 449-457.
Datta, J., Palmer, M. J., Tanton, C., Gibson , L. J., Jones, K. G., & Macdowall, W Johnson, A. M. (2016). Prevalence of infertility and help seeking among 15 000 women and men. Human Reproduction, 31(9), 2108-2118.
Dural, O., Yasa, C., Keyif, B., Celiksoy , H., Demiral, I., Yuksel Ozgor, B., & Bastu , E. (2016). Effect of infertility on quality of life of women: A validation study of the Turkish FertiQoL. Human Fertility, 19(3), 186-191.
Endler, N. S. & Parker, A. (1999).Coping inventory for stressful situations. North Tonawanda,NY: Multi Health System.
Fisher, J., & Hammarberg , K. (2017). Psychological aspects of infertility among men. Endocrinology of the Testis and Male Reproduction, 1(3), 1-31.
Ibrahim, E., Brackett, N. L., & Lynne , C. M. (2016). Advances in the management of infertility in men with spinal cord injury. Asian Journal of Andrology, 18(3), 382-390