EXPECTATIONS OF PATIENTS TOWARDS HEALTHCARE: A CASE STUDY OF NIGERIA AND CANADA
*Adeola Aminat Odebode, PhD and Falilat Anike Okesina, PhD
University of Ilorin, Nigeria
This study investigated the expectations of patients in Nigeria and Canada towards healthcare. The relationship of age and gender with expectation of healthcare was also explored. The descriptive research design was adopted for the study. The sample consisted of two thousand and four hundred respondents who were selected from both countries (Nigeria and Canada) using simple random, purposive and systematic random techniques. A new questionnaire entitled “Expectations of Patients towards Healthcare Questionnaire” (EPHQ) was developed and used in the studyto address the research questions and hypotheses. The validity of the scale was achieved through team of experts and the split half reliability of the instrument was .67. The data collected was analyzed using frequency counts, percentages, facto analysis t-test and Analysis of Variance (ANOVA). The results showed that there wasa significant difference between expectations of patients in Nigeria and Canada towards healthcare based on age and gender. It was concluded that Pan African and Canadian policies, processes and programs to further empower and sustain healthcare systems for the future, should be well structured to meet patients’ expectations.
Keywords: Expectations, Patients, Healthcare, Nigeria, Canada.
It is important to assess patients’ expectations toward healthcare to deliver a high-quality health care. Patients’ expectation is an issue that care providers need to address to ensure that patients are satisfied. With reference to healthcare, patients’ expectation refers to what patients hope to meet in the hospital in terms of the kind of care they receive, health care environment, kindness and politeness of care providers towards them. Patients’ expectations of the care they receive is key to health outcomes; this could be why patient satisfaction has been given considerable attention in the review of the National Health Service. Patients’ satisfaction is intertwined with patients’ expectation, health care providers and service factors (Kinnersely, Anderson, Parry, Clement, Archard, Turton, et. al., 2000).
Researchers such as Bryan-Brown and Dracup (1996) speculated that patients’ expectation of care, has a strong impact on their satisfaction. Invariably, though patients with extraordinarily high expectation were less satisfied with a high quality care while, those with low expectations were satisfied with deficient care (McKinley, Stevenson, Adams & Manku-Scott, 2002). Patients’ expectation varies according to age, gender, cultural group and educational status (Kinmonth, Woodcock, Griffin, Spiegal & Cambell, 1998). Nearly all patients assessing healthcare have certain level of expectations and reactions to unmet expectations can range from disappointment to anger (Lateef, 2013). However, understanding and proper management of patients’ expectations lead to gratification of a need and patients are usually grateful and satisfied (Hoy, 2008).
Most patients expect healthcare organizations to be clean, consulting rooms to be comfortable and providers to be competent (Michelle, Goertzen, Hutchison, Kaczorowski&Morris, 2007). According to Bowling etal. (2012), patients have diverse types of expectations (e.g. desires or predictions) and these expectations can be met through healthcare structures (e.g. building, equipment, staff) processes (e.g. waiting lists, the way staff and patients interact) and health outcomes (e.g. the effects of the health service on patients’ assessment of their health). In the opinion of Lim and Tang (2000), patients expect in health care system tangibility, reliability, responsiveness, assurance, empathy and accessibility and affordability.
Most patients accessing healthcare expect immediacy, personalized treatment and involvement in theirtreatment plan (Rappleye, 2015). In the submission ofMcKinley, Stevenson, Adams and Manku- Scott (2002), patient’s expectations revolve round domiciliary care, less waiting time and adequate advice from healthcare providers. Usually, patients come in to the hospital with fear and worry therefore, they expect that providers are helpful, compassionate, listening, responsive and reassuring; they expect that the environment should be clean and calm, smooth and confident procedure and that recovery is pain free (Lewis, 2013). Damouni (2013) posited that most patients expect healthcare organizations to be clean, rooms to be comfortable, less waiting time, providers must be competent and react in a timely manner. In the opinion of Doulgeris (2011), patients generally expect new and better drugs, efficient staff, up to date equipment, portable medical records, good accessibility of health care, effective communication channel between providers and patients and personalized care. These expectations seem to cut across patients and countries.
Nigeria is ranked among the 20th most developed economies but Nigeria, like other Sub-Saharan African nations is still far behind in most indices worldwide. For instance, Nigeria leads the World in malaria as it contributes to 25% of the global burden of disease. It is the second most burdened nation globally with HIV/AIDs (National Mirror, 2014). Nigeria harbors tuberculosis, polio, cancer, diabetes among others which has led to the death of several thousands of her citizens. Nigerians no doubt, expect service-driven healthcare institutions. Many States in Nigeria especially in the North, do not have sufficient healthcare services while personnel are acutely lacking in available facilities. Nigerians expect functional, well equipped health institutions to further help in reducing maternal/mortality and other preventable deaths. Eradication of quacks, strong primary and secondary level of care, ethical conducts among health workers to mention a few (National Mirror, 2014).
A report on Canadians’ expectations of the healthcare system revealed that 70% of Canadians are worried about falling through the cracks especially when it comes to critical areas such as mental care of seniors, palliative care and hospital safety (Health Care CAN, 2015). In the report, Canadians expect updated healthcare facilities, high quality mental healthcare, care of the seniors before they fall into crisis and palliative care. A 2014 report by the Common Wealth Fund showed that out of 11 developed countries, Canada’s healthcare system ranked 10th. Issues impacting Canada’s low score included the safety, timeliness and efficiency of care. In the common wealth surveys, the only factor in which Canada scored high is cost in which it was 5th out of 11 which implied that health care service in Canada is somehow not expensive. However, Canadians expressed that cost is not the only or even the most prominent issue (Health Care CAN, 2015).
Problem StatementWorldwide, hospitals are increasingly aware of the need to concentrate on quality service to improve and sustain the society. it is rather unfortunate that Nigerians seek medical care abroad, they migrate in mass out of Nigeria giving reasons such as searching for good jobs, good living condition and above all good medical care. To buttress this statement, as at the time of this study, the president of Nigeria is out of the country to seek adequate medical attention Oversea. It has been observed that the migration rate of people to Canada is on the increase. One would wonder why the rush to Canada? Could it be that they seek for better living condition or due to health expectation which could not be met in Nigeria? It is on this note that this study examined the health care expectations of patients in Nigeria and Canada. This study would ensure that patients’ expectations are continually assessed and well managed by health workers. The Government of both countries would be able to determine through the findings of this study, the priority of patients’ expectationsand what measures could be adopted to ensure that patients are satisfied.
Theoretical Basis of the Study
Expectancy Model/Theory.The basis for expectancy models has been made by Tolman (1932) and Lewin (1938). The model was influenced by Lewin's field theory because it involves the perceptual analysis of (1) alternatives with their (2) desirability and (3) expectancies, and their (4) outcomes in the immediate psychological field. Expectancy theory stated that the desire or motive to engage in a certain behavior is a composite of the expected outcome of that behavior and the value or evaluation of that behavior. The motivational force to engage in a behavior, as applied in organizational psychology, is a function of the four factors stated above (Vroom, 1964; Green, 1969; Porter & Lawler, 1968; Campbell, Dunnette, Lawler & Weick, 1970). However, it needs to be pointed out that the expectancy concept is not without questions. Firstly, the extension of the concept of "evoked set" (Howard & Sheth, 1969) seems to provide an answer to the question of how many alternatives, as well as types of alternatives are considered by the individual. Secondly, the desirability or attractiveness of the alternatives is a function of the probability that the alternative possesses a certain attribute times the evaluation of that attribute on a bipolar favorable- unfavorable scale. Third, Jacoby (1976) emphasized not overlooking the desired outcomes of a behavior as they are influenced by "motivational inputs". A distinction is made between input and output. "Outputs or outcomes refer to the primary functional aspects of the alternatives in the product set; they are the basic purpose for buying and using the product. Inputs, on the other hand, are those motivational forces other than perceived functional consequences which influence the selection of one specific behavioral alternative over the other available alternatives" (Jacoby, 1976).
If the functional goal of the purchase of a car is its service and economy, say, as opposed to status or a combination of all these, then these consequences constitute the desired outcomes. The inputs such as advertising, availability of deals, past satisfaction with the product, which is referred to as "antecedents" (Jacoby, 1976), may induce the consideration of one brand over another. Jacoby suggested the partitioning of the evaluation component into input (or antecedent) and output (or consequent) "values". Unfortunately, this is only at the brand level, and even at that level, it fails to resolve several questions raised earlier.
Vroom’s (1964) expectancy theory has held a major position in the study of work motivation (Van Eerde & Thierry, 1966). Also, known as Valence, Instrumentality, Expectancy (VIE) theory, examined the relationship between worker motivation and each of these three components. According to Vroom (1964), valence refers to the perceived value of an outcome (such as the perceived value of health care outcomes). For example, if a worker does not value a reward then they will be less likely to improve performance to attain the said reward. The concept of instrumentality refers to the perceived likelihood that one outcome will lead to another (e.g., that greater rewards will result in greater job satisfaction). Lastly, expectancy refers to the perceived likelihood that a behavior will lead to an instrumental outcome (e.g., going to the hospital will bring relief).
Expectancy theory showed a strong relationship between rewards and the amount of work needing to be done to achieve the reward. According to Vroom’s (1964) theory, an employee will exert more effort when they believe that their increased effort will result in a positive reward. For instance, if an employee believes they will receive a pay raise or a promotion if they receive a positive performance appraisal, they will be motivated to improve their overall job performance. However, if the employee receives no reward following a positive appraisal, they will be demotivated to continue performing at a higher level. Expectancy theory holds that individuals seek to maximize their positive outcomes. Expectancy theory emphasized self interest in the alignment of rewards with employee's wants. Expectancy theory argued that the strength of a tendency to act in a certain way depends on the strength of an expectation that the act will be followed by a given outcome and on the attractiveness of that outcome to the individual (Vroom, 1964). The Expectancy theory suggested that the individual may increase her performance if he perceives the outcome strongly to be desirable.
Objectives
- To investigate patients’ expectations towards healthcare in Nigeria and Canada.
- To find out the gender differences in patients’ expectations towards health care in Canada and Nigeria.
- To find out the differences in patients’ expectations towards health care on the basis of age in Canada and Nigeria.
- There is likely to be a difference in expectations of patients towards health care in Canada and Nigeria.
- There is likely to be a gender difference in the expectations of patients towards healthcare in Canada.
- There is likely to be a gender difference in the expectations of patients towards healthcare in Nigeria.
- There is likely to be a difference in the expectations of patients towards healthcare in Canada based on of age.
- There is likely to be a difference in the expectations of patients towards healthcare in Nigeria based on age.
Method
Research DesignDescriptive survey research design was adopted for the study. Descriptive survey methods give the researcher opportunity to describe, find out the attitude or expression of people towards events and ideas. Descriptive survey gives room for generalization of the entire population. It is in view of these, that the researchers adopted the descriptive method as appropriate for this study.
Sample Description and Selection
The sample comprised of 1800 participants including 900 from Canada and 900 from Nigeria. The sample age range was 18 to 60 years. Data collection was carried out in systematic way. In Nigeria, there are six geo-political zones out of which a zone was randomly selected. The south west zone that was selected comprises of six States; Oyo State was chosen, using the simple random sampling technique. This state has only one teaching hospital: The University College Hospital Ibadan, Nigeria. This University College Hospital is a tertiary institution with appendages of community based outreach activities and over One million domestic and international patients use this facility. The clinic at the General Outpatient Departments (GOPD) of the hospital was also purposively chosen for the study because it represents the primary health care section of the Hospital. The systematic random sampling technique was however, adopted to select every 20th patient that registered at the health record was sampled. If a patient did not consent, the next patient in line was chosen. This continued until 1200 respondents were selected from the Teaching Hospital. The patients were sampled across ages and gender. The study was conducted in Nigeria between January to June 2015.
In Canada, there are ten provinces; a provinceSaskatchewan was randomly chosen. This province has fourteen cities out of which one city was again randomly selected. In Regina city of Saskatchewan, there is only one general hospital; Regina General Hospital which is one of the region’s two major hospitals and has a long history of providing innovative and progressive institutional health care to the southern Saskatchewans. The Systematic Random Sampling Technique was used to select every 20th patient who attended the hospital and who consented to participate in the study. This continued until 1200 participants responded to the questionnaire. The respondents were sampled across ages and gender. The study was conducted in Canada between June to November 2016. The age of respondents was 18 years and above. Critically ill patients were not included in the sample.
Scale DevelopmentThe instrument titled Expectations of Patients towards Healthcare Questionnaire (EPHQ) was developed by the authors after extensive literature review. The authors are aware of various measurements of patients’ expectations of healthcare but many of these instruments yielded confusion over the terms experience, perception, expectations and satisfaction (Foundation, 2013; Sofaer & Firminger, 2005). Secondly what constitutes quality within existing instruments, was lacking the patients’ perspectives (Michelle, Lauder, Atherton & Murphy, 2001) and many of these instruments are not usable in real word of practice (Lynn, McMillen &Sidani, 2007). EPHQ contained 25 items that seek information on the expectations of patients at various levels of the healthcare system for instance, ‘I expect to meet in the hospital: clean environment, friendly staff, functional facilities’ etc. the respondents are required to respond on “yes” or “No”, which is then scored using percentages and Factor Analysis.
The validity of EPHQ was obtained by giving the instruments to team of experts both in Nigeria and Canada. These experts affirmed that the instrument has face and content validity. However the suggestions of the experts were incorporated.
The reliability of the questionnaire was determined using a split- half reliability procedure. The instrument was administeredon 20 patients in each country. The result was divided into two equal halves and was correlated using Cronbach Alpha formula. The correlation co-efficient obtained was 0.66 in Nigeria and 0.69 in Canada. The average reliability score was 0.67 (0.66+0.69/2). This indicated a positive and high correlation between the responses at the period of administration. The co- efficient was considered high enough to conclude that the instrument was reliable. Demographic form.The demographic form was used to collect personal information of the participants such as Age range (18- 27years; 28-37 years; 38-47 years & 48 years and above).
ProcedureEthical clearance was obtained from the Ethical Committee of the University College Hospital Ibadan. The researchers got clearance from the Ethical Review Committee (ERC) from the hospital. After completing the Citi Programme Course on www.citiprogram.org, and obtained a certificate. The researchers therefore proceeded to administer the questionnairesto the respondents. Research assistantswere recruited and trained for the study in Ibadan, Nigeria. The questionnaires were administered personally by the researchers in Canada. A total number of 1200 copies of the questionnaire were administered to the respondents in each of the countries to cater for loss and wrongly filled questionnaire forms.In Nigeria, 960 questionnaires were correctly filled and returned (80.50 % response rate) while in Canada 933 questionnaires were returned (77.75% response rate). The overall response rate for both countries was 79.12%. After data collection, only 900 correctly and completely filled questionnaire forms in Nigeria and Canada were analyzed using SPSS. This made a total of 1800 copies of the questionnaire forms that were used for analysis. All the results were reported accurately.
Results
The purpose of the study was to investigate the expectations of patients towards healthcare in Nigeria and Canada on the bases of age and gender. The descriptive statistics of the sample are presented in table 1.
Table 1 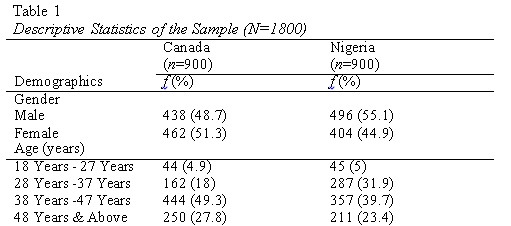
It was hypothesized that there is likely to be a difference in expectations of patients towards health care in Canada and Nigeria. To check the differences Independent Sample t-test was run. The results are presented in the table.
Table 2 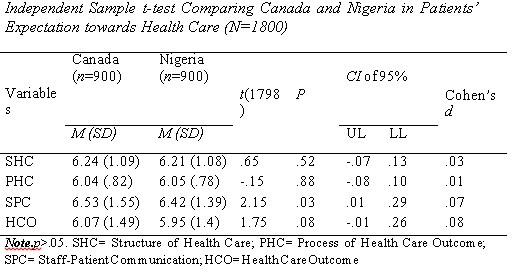
The Results showed significant differences in Staff Patient Communication in Canada and Nigeria. The mean differences showed that patients in Canada have higher expectations in Staff Patient Communication (M=6.53, SD= 1.55) than in Nigeria (M=6.42, SD=1.39). However, other domains of patients’ expectations towards health care showed non-significant differences in Canada and Nigeria.
It was hypothesized that there is likely to be a gender difference in the expectations of patients towards healthcare in Canada. To check the differences Independent Sample t-test was run. The results are presented in the table.
Table 3 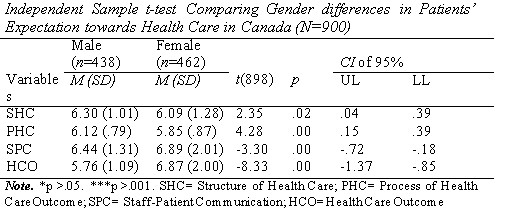
The table showed significant gender differences in all the domains of Patients’ expectations towards health care in Canada. Results indicates male respondents have higher expectations in Structure of Health Care (M=6.30, SD= 1.01) than female respondents (M=6.09, SD=1.28), Males respondents have higher expectation in process of health care (M=6.12, SD=.79) than female respondents (M=5.85, SD=.87). Moreover results also indicates that female respondents have higher expectations in staff patient communication (M=6.89, SD= 2.01) than male respondents (M=6.44, SD= 1.31) and also female respondents have higher expectations in Health Care Outcome (M=6.87, SD= 2.00) than male respondents (M=5.76, SD=1.09).
It was hypothesized that there is likely to be a gender difference in the expectations of patients towards healthcare in Nigeria. To check the differences Independent Sample t-test was run. The results are presented in the table.
Table 4 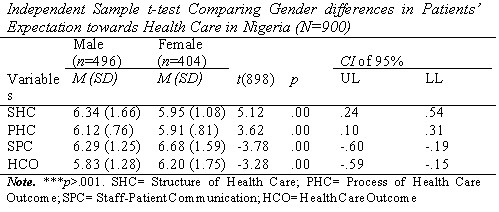
The table showed significant gender differences in all the domains of Patients’ expectations towards health care in Nigeria. Results indicates male respondents have higher expectations in Structure of Health Care (M=6.34, SD= 1.66) than female respondents (M=5.95, SD=1.08), Males respondents have higher expectation in process of health care (M=6.12, SD=.76) than female respondents (M=5.91, SD=.81). Moreover results also indicates that female respondents have higher expectations in staff patient communication (M=6.68, SD= 1.59) than male respondents (M=6.29, SD= 1.25) and also female respondents have higher expectations in Health Care Outcome (M=6.20, SD= 1.75) than male respondents (M=5.83, SD=1.28).
It was hypothesized that there is likely to have significant differences in Patients’ expectations towards health care in Canada based on age. One way ANOVA was run to investigate this. The results are presented in table 5.
Table 5 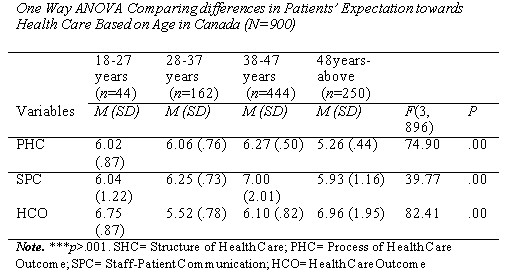
The results showed significant differences in all the domains of patients’ expectations towards health care in Canada based on age. The results of post hoc showed that the age group of 48 years and above were higher in structure of health care (SHC) and health care outcomes (HCO) domains of patients ‘expectations towards health care than 18- 27 years and 28-37 years groups. However the age group of 18 years – 27 years was higher than other groups in process of health care (PHC) and health care outcome (HCO) domains of patients’ expectations towards health care.
It was hypothesized that there is likely to significant differences in Patients’ expectations towards health care in Canada based on age. One way ANOVA was run to investigate this. The results are presented in table 6.
Table 6 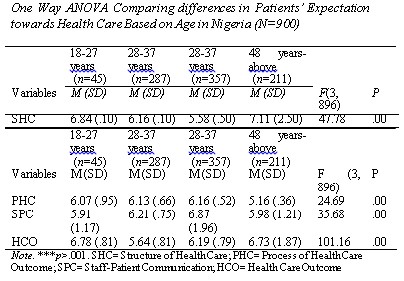
The results showed significant differences in all the domains of patients’ expectations towards health care in Nigeria based on age. The results of post hoc showed that 18- 27 years group was higher in structure of health care (SHC), health care outcome (HCO) and process of health care (PHC) domain of patients ‘expectations towards health than all other groups. However, the group of age 48years –above was higher in staff patient communication (SPC) domain of patients’ expectations towards health care in Nigeria.
Discussion
The findings suggested that health care expectations of respondents showed differences in staff-patient communication in Canada and Nigeria. These findings are consistent with the theoretical basis/submissions of Vroom (1964) and Jacoby (1976). Vroom believed that an individual will prefer certain things when they hope that those things will yield positive results. Similarly, Jacoby asserted that earlier satisfaction may prompt individuals to choose/expect one alternative over the other alternatives.
Moreover, all the respondents expressed that they expect helpful and friendly reception staff, understanding and accommodating nurses, compassionate pharmacists, polite and reassuring physicians and that they themselves get involved in their treatment plan. This finding tally with that of Doulgeris (2011) who found that patients generally expect efficient staff and maintenance of effective communication channel between providers and patient and personalized care. The finding also corroborates the findings of Lewis (2013) who ascertained that patients expect that providers are helpful, compassionate, listening, responsive and reassuring. Attending to patients with compassion, listening attentively to patients, being polite to patients, assuring patients and getting patients aware and involved in their treatment is key to the provision of quality care; this could be the reason for the trend of the finding of this study.
The findings highlighted significant difference in the expectations of patients towards healthcare in Nigeria based on gender. This also implies that in Nigeria, male and female have differed health care expectations. This finding is not consistent with the findings of Odebode, Adegunju and Shuaib (2016) and Taylor, Keneddy, Virtue and McDonald (2006) which showed that majority of patients have similar health care expectations. Again, this finding is against the submission of expectation theorists that many individuals seek and expect satisfaction in whatever they engage in, irrespective of gender.
The findings suggested significant difference in the expectations of patients towards healthcare in Canada based on of gender. What this connotes is that male and female in Canada expressed different health care expectations. The reason behind this finding could be due to different gender roles in the society which can affect one’s expectations. There is every tendency that the female respondents expect more out of healthcare because they have more health issues to battle with, an example is pregnancy and child birth. This finding does not support the findings Liyasu, Abubakar, Abubakar, Lawan and Gajida (2010) who found out that gender is not a yard stick for measuring health care issues.
Furthermore, the testing of the hypotheses revealed that there is a significant difference in the expectations of patients towards healthcare in Nigeria based on age. This implies that age influenced the expression of health care expectation of the respondents in Nigeria. The result further showed that respondents in Nigeria between 48 years and above contributed most to the differences noted. Similarly, the testing of the hypotheses revealed that there is significant difference in the expectations of patients towards healthcare in Canada based on age. This implies that age also influences the expression of health care expectation of the respondents in Canada. Surprisingly, respondents who are at the extreme ends of adulthood (early adulthood and late adulthood), contributed to the differences in health care expectations in both countries. The trend of this result could be that these categories of respondents seek health care services more especially at childbearing and old ages where numerous psychological and health challenges are at their peak. This finding is consistent with the findings of McNaughton, Mitchell, Hernadez, Padilla, and Bladon (2006) which agreed that patients differ in their expectations of healthcare based on age.
Recommendations
Based on the conclusion of this study, it is therefore recommended that both countries should ensure that patients’ expectations are constantly met by providing adequate healthcare structure such as conducive waiting and consultation rooms. Pan African and Canadian policies, processes and programs to further empower and sustain healthcare systems for the future should be well structured to meet patients’ expectations. Healthcare professionals should also be employed and well remunerated particularly in Nigeria, to care for the Nigerian population. Hospital administrators must make the health process friendly to patients to enhance patients’ satisfaction. Strict monitoring of the process should be in place for compliance. Curriculum of health providers should be revised to encompass the expectations of patients. Health care Professionals need to open effective communication line for patients; they should exercise patience with them, be compassionate, reassuring and timely in attending to them. Patients’ experience and perceptions of healthcare should be assessed continuously to provide meaningful service that will meet their expectations in both countries.Professionals should ensure that they give quality treatment to patients that will improve quality of life, have low complications and side effects.
References
Bowling, A., Rowe, G., Lambert, N., Waddington, M., Mahtani, K. R., Kenten, C., Howe, A. &Francis, S. A. (2012).The measurement of patients' expectations for health care: a review and psychometric testing of a measure of patients' expectations. Health Technological Assessment, 16(30), 501-509.
Bryan-Brown, C.W. & Dracup, K. (1996). Outcomes, endpoints, and expectations. American Journal of Critical Care, 5(2), 87-89.
Doulgeris, J. (2011). Top 10 Changes in Patient Expectations (Part II). Retrieved 12th fromhttp://www.physicianspractice.com/blog/top- 10-changes-patient-expectations-part-ii.
Graen, G.B. (1969). Instrumentality theory of work motivation: some experimental results and suggested modifications. Journal of Applied Psychology Monographs, 53(2), 112-122.
Healthcare CAN (2015). Situation critical: Canadians give healthcare system a failing grade. Retrieved from Canadians-expectations- of-the-healthcare-system/.
Kinnersley, P., Anderson, E., Parry, K., Clement, J., Archard, L., Turton, P., et al. (2000). Randomised controlled trial of nurse practitioner versus general practitioner care for patients requesting “same day” consultations in primary care. British Medical Journal, 320 (7241), 1043-8.18.
Jacoby, J. (1976). Consumer and industrial psychology: prospects for theory corroboration and mutual contribution," in D. M. Dunnette (ed.). Handbook of organizational psychology.
Kinmonth, A.L., Woodcock, A., Griffin, S., Spiegal, N. & Campbell, M.J. (1998). Randomised controlled trial of patient centred care of diabetes in general practice: impact on current wellbeing and future disease risk. British Medical Journal,317, 1202–1208.
Lim, P.C. &Tang, N. K. (2000). A study of patients' expectations and satisfaction in Singapore hospitals. International Journal of Health Care & Quality Assurance, 13(6-7):290-299.
McNaughton, H.L., Mitchell, E.M.H., Hernadez, E.G, Padilla, K. & Bladon, M. M. (2006). Patient privacy and conflicting legal and ethical obligations.American Journal of Public Health, 96(11), 223-237.
Michelle, H.,Goertzen, J., Hutchison, B., Kaczorowski, J. &Morris, K. (2007). Patient satisfaction with care for urgent health problems: a survey of family practice patients. Annals of Family Medicine, 5(5), 419-424.
National Mirror (2014). Nigeria’s healthcare: High expectations for 2014. Retrieved fromhttp://nationalmirroronline.net/new/nigerias- healthcare-high-expectation -for-2014/.