Centre for Clinical Psychology, University of the Punjab Lahore, Pakistan
The present study aimed to explore quality of life and death anxiety among patients with cancer and non-cancer participants. Between group research design was used in the present research. This study was conducted on 105 patients with cancer and 95 non-cancer participants. Data of patients with cancer was collected from the outdoor as well as indoor departments of Oncology of 3 teaching hospitals and 2 private hospitals and 3 private clinics. The patient’s population was taken after complete diagnosis by respective doctors while the non-cancer participants were taken from the community. Death anxiety was measured through the Leming fear of death anxiety scale, (Leming, 1980) and Quality of life was assessed with the help of World Health Organization quality of life scale- BREF (World Health Organization, 1991). Cancer and non-cancer participants groups were matched on age, gender, education, socioeconomic status, occupation, and religion. The results of t-test indicated that cancer patients had higher level of death anxiety while significance difference between the Quality of life among patients with cancer and non-cancer participants except social relationships. Using one way ANOVA, significant differences of death anxiety were found on the basis of level of religiosity among Patients with cancer and non-cancer participants were found in which patients with cancer had greater level of death anxiety as compared to non-cancer participants while opposite was true for level of religiosity. The results were discussed in the light of previous literature and theoretical background.
Keywords: Quality of Life, Death Anxiety, Patients with CancerIt is commonly believed that normal people are afraid to die and that death anxiety is a culturally universal phenomenon. As a result,
some people assume that the threat of death will serve as a deterrent to the kind of behavior that is deemed to be undesirable, inappropriate, and/or threatening to the society. The experience of death fear is associated with age, gender, and occupation. Older people tend to have less death anxiety (Gonen et al., 2012). Another study has concentrated on gender differences in death anxiety, documenting that men and women have different types of fears related to death, in general and women tend to fear death more than men (Dennis, 2009). Writers have generally agreed that the term fear is used when the negative reaction is to some known cause while anxiety is a term reserved to indicate a reaction to some unknown cause. Death anxiety is the phenomenon stating that death is basically an unknown experience; fear of death is a frequent label as well, perhaps suggesting that the fact of death, if not the actual experience is known (Leming, 1980; Dennis, 2009).
The model of death anxiety is based on Regret Theory by Tomer and Eliason (1996) postulate three immediate antecedents of death anxiety: past related regret, future related regret and meaningfulness of death. Past related regret refers to a person’s unfulfil ed aspirations that should have been achieved but were not. Future related regrets refer to the anticipation that as a result of premature death one cannot achieve important goals in future. Meaningfulness of death refers to one’s concept of death and ability to make sense of it. If the person desires or the goals remained unfulfilled then the death anxiety would increase near the old age.
Tomer and Eliason (1996) cited that Wong, Reker, and Gesser (1994) conceptualized death acceptance which include three components: natural acceptance approach, acceptance to beliefs in afterlife and escape acceptance (death as an alternative to miserable life). It is important to realize that belief in an afterlife or immortality is one way to think about death as meaningful. Alternative ways may be related to a process of de- individualization in which the self tends to transcend its boundaries reuniting with the universe (Jenko, Gonzalez, & Seymour, 2007). Apart from this, another major concept was given by Lewis and Butler. According to them, it is not the fear of death that af ects the person’s life but it is the fear of the belief in the meaninglessness in the life that has been spent when a lot of purposeful things could have been done (Taylor, 2003). The individuals who think that their life was spent aimlessly are more worried about death while individuals with meaningful life experiences show acceptance towards death. Another way in which death can be meaningful is as an escape from a miserable life. Indeed there a
negative correlation between escape acceptance and fear of death was found (Wong, Recker, & Gesser, 1994 as cited in Neimeyer, 1998).
Meaningfulness of death is determined by one’s beliefs about the world and about its self. In order to clarify this point, Antonovski’s sense of coherence model (Antonovski, 1987 as cited in Tomer & Eliason, 1996), postulates the existence of three components: comprehensibility manageability and meaningfulness. The first component refers to the perception of the world as structured, predictability explicable. The other two components are self-related, dealing with an individual’s perception of self as resourceful and able to find meaning in life demands. All three components may affect the way death is being perceived (Tomer & Eliason, 1996). In this model self-esteem is included in “beliefs about the self” and is related to death anxiety mainly by affecting the two types of regret. It was also suggested that older people have lower level of death anxiety. Older people are more likely to be overwhelmed by personal losses and physical illnesses. It was also found that women are generally more fearful of death as compared to men as they are more open to discuss their issues related to death (Taylor, 2003). The members of families that are not well settled would have greater threat of death as compared to heads of families who are well adjusted.
Death anxiety is an important aspect of every individual’s life. Individuals with terminal illness such as cancer tend to have more death anxiety then other people (Cohen, 2014). Cancer is a disease of cells. It is an abnormal growth of cells which tend to proliferate in an uncontrollable way and in some cases to metastasize (spread). Death anxiety is a common reaction to cancer. One may experience anxiety when undergoing a cancer screening test, waiting for the test results, receiving a diagnosis of cancer or anticipating the reoccurrence of cancer. Anxiety associated with cancer may increase feelings of pain, interfere with one’s ability to sleep, cause nausea and vomiting and interfere with the patient’s (and his family’s Quality of Life). Moreover, Khalid (1990) found that cancer patients were significantly more depressed and anxious than the patients suffering from other diseases or no disease. If left untreated severe anxiety may even shorten a patient’s life (Taylor, 2003). Quality of life is considered an attitude that is rooted in cultural beliefs. It is assumed to change with the growth and development of the individual. It is reflected in the expression of feelings, emotions and behaviors and is considered as set criteria against which choices are made from several options (Singer & Martin, 1999).
Wish for death in terminal illness has been a focus of previous researches. Wilson et al (2000) examined the desire for death among cancer patients. Cross-sectional survey was done and data was collected from eight Canadian palliative care programs. 377 patients with cancer were recruited in the study. Desire for Death Rating Scale and Structured Interview of Symptoms and Concerns were used for the data collection. Almost 68% patients had no wish to die. About 19% acknowledged occasional thoughts of death, and about 12% reported that they want to die. In the latter group, 24 individuals (52.2%) were diagnosed with a mental disorder and 22 (44.8%) were not. The subgroup of patients with a serious desire for death but no concurrent mental disorders still reported increased distress due to physical symptoms and social concerns. Moreover, Vander Lee, Vander Bom, Swarte, Heintz, De Graeff, and Van Der Bout (2005) conducted a study the association between depression and the incidence of explicit requests for euthanasia in terminally ill cancer patients. A prospective cohort study was conducted on 138 consecutive cancer patients with an estimated life expectancy of 3 months or less. At inclusion, participants completed the Hospital Anxiety and Depression Scale. To identify "depressed mood" cutoff score of 20 was used. Kaplan-Meier curves and Cox regression analyses were used to assess the association between depressed mood and the risk of a request for euthanasia. Among 138 patients, 32 patients had depressed mood at inclusion. Thirty patients (22%) made an explicit request for euthanasia. The risk to request euthanasia for patients with depressed mood was 4.1 times higher than that of patients without depressed mood at inclusion.
In explaining other factors which affect death anxiety and quality of life of the individuals with terminal illness, Montazeri, Hole, Milroy, and Gillis (2003) found that the patients who were deprived of basic health care facilities had lower health-related quality of life. Role of social support in the recovery and life expectancy of the cancer patients was significant as evidenced by empirical evidence. On the other hand religion was also significantly related to general satisfaction with life and feelings of hopelessness. Depression in cancer patients with an estimated life expectancy of less than 3 months is associated with a higher likelihood to request for euthanasia (Neimeyer, 1994). Canada, Murphy, Fitchett, and Stein (2016) concluded faith as the significant contributors of the quality of life among cancer survivors provided that the life of the individual is thought to be peaceful and/or meaningful.
The objectives of the present research were to identify differences among the level of death anxiety and quality of life in patients with cancer and non-cancer participants and differences in death anxiety on the basis of level of religiosity in patients with cancer and non-cancer participants.
• There is a difference between the level of quality of life and death anxiety among patients with cancer and non-cancer participants. • People who are more religious are likely to have low death anxiety.
The present study used cross sectional research design for the exploration of the phenomenon
Purposive sampling were used to study the difference between the level of death anxiety among patients with cancer and non-cancer participants with reference to quality of life The subjects employed in the study were 105 patients diagnosed with cancer and 95 non-cancer participants with an age range of 25-70 years. Both in-door and out-door patients population were included in the study.
Demographic questionnaire. Two demographic questionnaires; one for the patients with cancer and other for non-cancer participants focusing on age sex, education, occupation, marital status, religion, monthly income, sources of monthly income, type of residence, area of house, no. of siblings, family system, relationship with parents, relationship with siblings and relationship with spouse, duration of illness, duration of diagnosis of illness, reaction towards illness, family reaction towards illness, sources of treatment, duration of treatment, type of treatment, sources of expenses on treatment, level of satisfaction to the treatment, reaction to treatment, family reaction to treatment, physical
complaints, previous physical illness, post psychological illness, previous psychological illness and physical, psychological as well as emotional well-being were developed.
Leming fear of death anxiety scale (Leming, 1980). It is 26- items instrument with response category of 6-point scale ranging from strongly agree to strongly disagree. The scale yields eight sub scores: Fear of Dependency, Fear of Pain, Fear of Indignity, Fear of Isolation, Separation, Loneliness, Fear of Afterlife Concerns, Fear of the Finality of Death, Fear of Leaving Loved Ones, and Fear of the Fate of the Body. Internal consistency for the eight sub scores for the present study were Fear of Dependency, .68; Fear of Pain, .53; Fear of Indignity, .55; Fear of Isolation, Separation, Loneliness, .72; Fear of Afterlife Concerns, .69; Fear of the Finality of Death, .79; Fear of Leaving Loved Ones, .51; and Fear of the Fate of the Body, .86. The Leming Fear of Death Scale was translated using forward and back-translation procedure.
Australian world health organization quality of life scale (WHO, 1991). The Australian World Health Organization Quality of life (WHOQOL) contains 26 items. Four types of scales are used to assess intensity, frequency, capacity and evaluation. The correlation coefficients were calculated for each domain (i.e. physical domain =.85, psychological domain =.83. social relationships =.84, environment =.83
and .57, .67 for item number 1 and 2 respectively (Taylor, 2003).
Permission was sought from the relevant hospitals. Permission to use and translate the research questionnaires was also sought. Informed consent was taken and information sheet including the rights and responsibilities was provided. Confidentiality was assured to all the research participants before conducting the research. All the research participants had the right to withdraw from the research at any point of time.
Pilot study. A pilot study was conducted on 3 patients with cancer and 3 non-cancer participants. The main purpose to conduct the pilot study was to figure out the total time to be taken for the administration and to measure their level of comprehension and fatigue. It took 15 minutes to administer the demographic questionnaire and 20 minutes to administration Leming fear of death anxiety scale and almost 15 minutes
to administer the Quality of Life Scale. The total amount of time taken for all the administration was approximately an hour for both groups.
Main study. The sample for the main study was 200 participants consisting of 105 patients with cancer and 95 non-cancer participants. The ratio of male and female was equally divided among two groups; patients with cancer and non-cancer participants. A written informed consent was signed by each participant, included information about the rationale of the study and it was also explained that the subject has the right to refuse to participate in the study at any point in time if any one of them desires to do so. The confidentially process was also communicated and it was also communicated that the information gathered through this process would be used only for research purposes.
Approval of Department Doctoral Program Committee was sought for conducting the research. Permission to use the questionnaires was taken from the respective authors. Permission from the hospital authorities was sought for collecting the data. Participants were assured about the confidentiality of their information. The participants were given the information sheet that included all information about the nature, purpose, procedure, duration of research, their role as research participants and contact of appropriate person in case of any difficult situation. Consent of the participants was obtained and in case of severe illness, pain or any other reason, they had the right to withdraw from the research at any time. The data was protected and entered in the computer program with codes and nobody other than the researcher and her supervisor had access to the collected data. Results were genuinely analyzed and reported without any fabrication or faking.
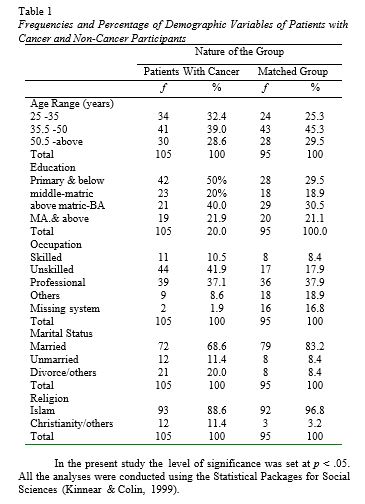
The present study compared the level of death anxiety among patients with cancer and non-cancer participants with reference to their Quality of Life. Both of these groups were matched on age, gender, education, socioeconomic status, occupation, and religion. The main hypotheses of the study were analyzed by using t-test and One Way of Analysis of Variance (ANOVA). The frequencies and percentages are calculated for the demographical variables and are presented in table.
The first hypothesis of the study was that there is a difference in the death anxiety among patients with cancer and non-cancer participants. To check the difference, t-test was performed.
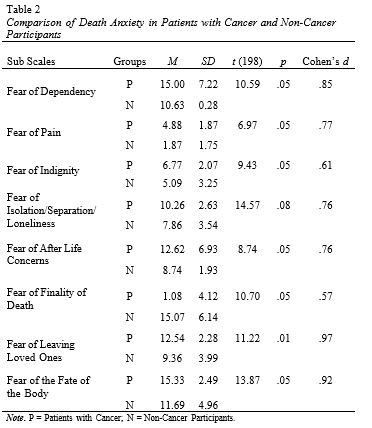
The table 2 shows significant difference between the level of death anxiety among Patients with cancer and Non-Cancer Participants. The results indicate that patients with cancer had higher level of death anxiety as compared to non-cancer participants. All the results were significant apart from the fear of isolation/separation/loneliness. It was also hypothesized that there is a difference in the quality of life between the patients with cancer and the non-cancer participants. To check the difference, t-test was performed. The table 3 is showing a significance difference between the Quality of Life among patients with cancer and non-cancer participants except social relationships.
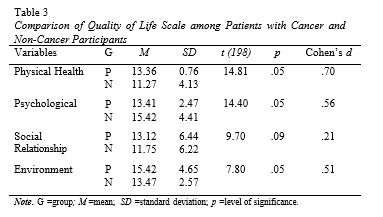
All the results were significant apart from the component of social relationship. However rest of the subscales showed significant difference of the Quality of Life among Cancer Patients and Non-Cancer Participants. Lastly, ANOVA was computed to check the difference between the Level of Death Anxiety and Level of Religiosity among Cancer Patients and Non-Cancer Participants. The results in table 4 reveal that there is significant difference between the Level of Death Anxiety and Level of Religiosity among Cancer Patients and Non-Cancer Participants.
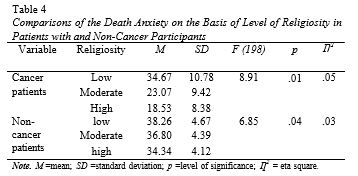
The results revealed that there was significant difference between the level of death anxiety and level of religiosity among Cancer Patients and Non-Cancer Participants.
The results are likely to be supported the main hypotheses of the research that there is a difference between the level of death anxiety among cancer patients and healthy individuals. The second hypothesis is also confirmed that the quality of life was affected in cancer patients as compared to non-cancer participants as reported greater dissatisfaction with their quality of life as compared to non-cancer participants.
The present study findings are consistent with the research conducted by Khalid (1990) in which it was examined how the patients suffering from cancer differ in their attribution to depression and anxiety. It was found that cancer patients were significantly more depressed and anxious than the patients suffering from other diseases or no disease. The results also showed the attribution of cancer patients was significantly more external than the non-terminal patients.
In the present study significant difference was found between religiosity and death anxiety among Non-Cancer Participants. The previous literature found that the more the person is religiously inclined the less would be his threat of death. According to Leming, the anthropologist Bronislaw Malinowski poses that religion functions to relieve anxiety caused by crisis. According to Malinowski, religion is the “great anxiety reliever” (Leming, 1980). This is exceptionally appropriate for the religiously oriented Muslim societies such as in Pakistan. A
research by Canada, Murphy, Fitchett, and Stein (2016) investigated religiosity, depression and anxiety in Muslim cancer patients. Fifty-nine participants were recruited from hospitals that completed the Muslim Religiosity and Personality Inventory, Beck Depression Inventory and Beck Anxiety Inventory. Results yielded negative correlation between religiosity with depression and anxiety. Older and married patients scored significantly higher on religiosity. Results provided an insight into the significant role of religious intervention which has huge potentials to improve the psychological health of cancer patients particularly Muslims in Malaysia. Similar conclusions were made by Gonen et al (2012) that death anxiety among cancer patients was significantly correlated with the symptoms of anxiety and depression, and fearful and negative beliefs about life after death. Unresolved life goals were found out to be directly related with the death anxiety. The patients who had spent meaningful life were less afraid of death as compared to those who had unresolved goals and conflicts.
This research would further help to develop plans and strategies to work with people who are terminally ill and also to develop effective strategies to enhance their quality of life. Overall it would also be helpful to take measures to improve the quality of life among individuals with cancer disease. It also stresses upon the planning for counseling services for people to understand their meaning in life (Gangdal & Inger, 1996; Vachon, 1994).
In this research the data was collected from 100 cancer and 100 non-cancer participants which may not be a representative sample of the overall population. The generalizability of the results in the use of self- report measure may lead to response bias. The cancer patients with severe illness were not included in the research due to ethical considerations. Most of the participants were taken from the urban areas this may also lead to the limitation to the generalization of the results to the rural population. To make the research more representative of the Pakistani population it is recommended that the sample should also include participants from rural areas.
Canada, A. L., Murphy, P. E., Fitchett, G., & Stein, K. (2016). Re- examining the Contributions of Faith, Meaning and Peace to Quality of Life: A Report from the American Cancer Society's
Studies of Cancer Survivors-II (SCS-II). Annals of Behavioral Medicine, 50(1), 79-86.
Cohen, M. (2014). Depression, anxiety, and somatic symptoms in older cancer patients: a comparison across age groups. Psycho Oncology, 23(2), 151-157.
Dennis, D. (2009). Living, dying, grieving. Tennessee: Jones & Bartlett Learning.
Gangdal, M. S., & Inger, G. (1996). Religiosity, quality of life and survival in cancer patients. Social indicators research. [Abstract]. Psychological Abstracts, 38(2), 193-211.
Gonen, G., Kaymak, S. U., Cankurtaran, E. S., Karslioglu, E. H., Ozalp, E., & Soygur, H. (2012). The factors contributing to death anxiety in cancer patients. Journal of Psychosocial Oncology, 30(3), 347-
358. Retrieved from http://www.clas.ufl.edu/users/ardelt/Role% 20of%20 religion.pdf
Jenko, M., Gonzalez, L., & Seymour, M. J. (2007). Life review with the terminally ill. Journal of Hospice & Palliative Nursing, 9(3), 159- 167.
Khalid, R. (1990). Depression, anxiety & attribution: comparative study of cancer and other patients. In M. H. Mubbashar, & A. R. Syed (Eds). Mental health for all, all for mental health (pp.75-81).
Leming, M. R. (1980). Religion and Death: A Test of Homans’s Thesis.
Omega, 10 (4), 347-364.
Montazeri, A., Hole, D. J., Milory, R., McEwen, J., & Gillis, C. R. (2003). Quality of Life in Lung Cancer Patients: does Socioeconomic Status matter? Health and Quality of Life Outcomes, 1(9), 19-24. Retrieved from www.hqlo.com/content/1
/1/9.
Neimeyer, R. A. (1988). Special article: Death anxiety research: The state of art. Omega: Journal of Death & Dying, 36(2), 163-169.
Neimeyer, R. A. (1994). The Threat Index and Related Methods.
Washington, DC: Otto Rank Association.
Singer, P. A., Martin, D. K. & Kelner, M. (1999). Quality end of life: parent’s perspective. Journal of American Medical Association, 13(2), 163-168.
Taylor, S. E. (2003). Health psychology (5th ed.). New York: McGraw Hill Companies. ADD.
Tomer, A., & Eliason, G. (1996). Towards a comprehensive model of death anxiety. Death Studies, 20(4), 343-365. Retrieved from www.ezonline.com/grafton/death.html
Vachon, M. S. (1994). Psychological Variables: Cancer morbidity and mortality. In I.B. Coreless, B. B. Germino, & M. Pittman (Eds.). Dying, death and bereavement: theoretical perspectives and other ways of knowing. Boston: Jones and Bartlett Publishers.
Van der Lee, M. L., Van der Bom, J. G., Swarte, N. B., Heintz, A. P. M., de Graeff, A., & Van den Bout, J. (2005). Euthanasia and depression: a prospective cohort study among terminally ill cancer patients. Journal of Clinical Oncology, 23(27), 6607-6612.
Wilson, K. G., Scott, J. F., Graham, I. D., Kozak, J. F., Chater, S., Viola,
R. A. & Curran, D. (2000). Attitudes of terminally ill patients toward euthanasia and physician-assisted suicide. Archives of Internal Medicine, 160(16), 2454-2460.
Wong, P. P., Reker, G. T., & Gresser, G. (1994). Death attitude profile- revised: A multidimensional measure of attitude towards death. In
R. A. Neimeyer (Ed.). Death anxiety handbook: Research, instrumentation and application. Washington, DC: Otto Rank Association.