Center for Clinical Psychology, University of the Punjab, Lahore The present research was conducted to find out distress in women with miscarriage and its relationship with religious rituals, spiritual and social support. It was hypothesized that social support, spiritual support, religiosity and number of miscarriages will likely to predict distress in miscarrying women. Correlatioal research design was employed. Sample selected 100 participants divided in two groups, 50 participants each group using purposive sampling. Sample was taken from two different hospitals of Lahore. Both groups were matched on age, education, income level, occupation, family system and number of children. Demographic questionnaire, Religious activity scale (RAS: Sitwat, 2005), Spiritual support scale (SSS; Maton, 1989), Multidimensional scale of perceived social support (MSPSS; Zimet et al., 1988) and Center for epidemiologic studies depression scale (CES- D; Radloff, 1977) were employed to assess religious activities, beliefs, social support and level of distress in miscarriage. Findings depicted that Social support, spiritual and number of miscarriages is related to distress in miscarrying women. Number of miscarriages and social support emerged as significant predictors of distress in miscarrying women. Religious activities and spiritual support were not significantly associated with the level of distress.
Keywords: Religiosity, Social Support, Distress, MiscarriageA woman in her life faces a lot of stressful and challenging events. One of such events includes loss of loved ones that causes distress which sometimes leads towards depression if not coped well. Loss of child or miscarriage in someone‟s life could be a distressing event and increases risk of depression (Conway, 1995). The present research focused to measure the level of distress in women who had a spontaneous abortion (miscarriage). Moreover, this study also explored the relationship of religious practices, spiritual support and social support with level of distress in women.
Miscarriage, still birth, birth loss, and medically based termination are four types of pregnancy loss. The most common is a miscarriage, which refers to any pregnancy loss that takes place before the 20th week in pregnancy (pregnancy typically lasts 40 weeks). The majority of miscarriages happen even earlier than that --usually before the 12th week or by the end of the first trimester (Bupa‟s health, 2009).
Physical effects of miscarriage involve little pain and in some cases pain do not occur at all. The effect of emotional distress and psychological problems in miscarriage is greater than physical impact. There are number of feelings that lead to miscarriage. Every one reacts according to their own habit and there is no right or wrong way to feel or behave (Bupa‟s health, 2009). A sma l portion of patient may experience pleasure at the loss if pregnancy is unwanted or they considered that they got rid of an abnormal pregnancy. The patient with the wanted pregnancy usually feels depressed (Chohan, 2005). Meeting with pregnant women and mother of new born children is often painful for parents who have experienced miscarriage. Sometimes this leads to difficulties in conversation with friends, acquaintances and icon of family (Howard, 2009).
It becomes problematic to accurately find out the prevalence of miscarriage as many miscarriages happen early in the pregnancy before a woman may get to know that she is conceiving a child. Women‟s treatments with miscarriage at home also create a hinder in having accurate statistics. Prospective studies using very sensitive early pregnancy test have found that 25% of conception are miscarried when the sixth week of pregnancy starts and from the moment of women last menstrual cycle (Lincoln, Chatters, & Taylor, 2005). This is obvious that loosing baby either through miscarriage or by any other source causes stress in the ones associated with the baby.
Every one experiences stress. It is not only common but also play positive role within acceptable limits. Nonetheless there is a difference between day to day stress (looking after children, work demands, transportation difficulties etc.) and distress. Stress may produce physical and nervous tension but is still able to cope with environment. When stress may exceed the required limit it may get converted in to distress.
Selye (1975) presented a model of stress which states that stress is divided in to eustress and distress. Where stress polishes function (physical or mental, such as through strength training or challenging work) it may be considered eustress. Continuous stress that is not
solved through coping or adaptation may lead to anxiety or withdrawal (depression) behavior (Howard, 2009). Distress may be defined as a condition in which coping strategies of individuals may begin to disrupt. Stress become distress when it is: not wanted, unaccepted, ongoing and because of serious life problematic events or situations (e.g. family aggression, death of family member, divorce, separation, a jail term, etc. And for thousands of years, people have turned to religion or spirituality as a way to reduce stress, anxiety, and bring warmth, comfort, and meaning into their daily lives. Some research has shown that praying or believing in God could actually reduce stress (Bushak, 2009).
English and English (1958) suggested that religion is a process of values, practices, rites, rituals, commemorations and beliefs by means of which person or a society keep themselves in relation to God or to a supernatural powers, and often to each other and contains a set of values by which to judge events in the natural world (as cited in Loewnthal, 2000). The word religion derived from Latin word Reigio, which is generally thought to be as obligation or bond and emphasizes belief in, compliance or and submission to the sacred divine (Quinn, 2005). A more appropriate working definition of religion is that offered by Argyle and Hallahmi (1975), namely that religion is a process of belief in pious or super human power, and performance of prayers or other rituals instructed towards such a power. Islam is a monotheistic religion, depicting that central focus is on oneness of God. In Arabic it means submission to the will of God. Hussain (1996) reported that prayer and other religious means lessen distress (as cited Loewntal, 2000). Islam has Sariah, a code for both spiritual and temporal life based upon the Quran and Sunnah (Fontana, 2003).
Glock and Stark (1975) depicted that religious activities consist of five domains or dimensions:
Spirituality is defined as attachment to the religious morals, or to things of the spirit which are in opposition to material or worldly interests (Merriam-Webster‟s Collegiate Dictionary, as cited in Learnwell, 2009). According to Quinn (2005), “Spirituality is considered as the condition, behavior or state of being devoted to God, religion or spiritual interest or values, as opposed with physical or materialistic interests and more specifically the religious way of life of certain personals and societies of weather religious doctrine or beliefs”. Sitwat and Anjum (2007) identified that religious practice and spiritual support was a protective buffer against anxiety and depression in high stress conditions in cancer patients. Social support gives people the feeling of being loved and cared for, esteemed and moral also gives moral attachment. It also allows an individual to accept as well as to give others confirmation, affirmation and help, especially during difficult times. Strong family relations and close bonds with friend‟s helps old people face with the life events commonly associated with aging, such as retirement, widowhood, disability related to mobility, and bad health (Howard, 2009). Conway (1995) conducted a pilot study with 24 women and finds that psychological high pitched sound following miscarriage found to be same to system of feeling sad and depress, while help can also be obtained from social support of partners, kinship members and friends (Conway, 1995). Research studies have shown that depressed people who have low social support remain depressed longer than those who have warm friends and family members (Moos & Cronkite, 1999). Samuel, Hyacinth, and Innocent (2008) conducted a study which revealed that presence of husband, parents, children and relatives, friends and religious practices were identified as positive coping strategies.
Miscarriage is a leading problem worldwide and increasing cause of distress in women. The prevalence of miscarriage in Pakistan is not exactly known (Conway, 1995). Moreover little has been studied on coping mechanisms involved in recovery from traumatic experience of miscarriage. Since in our culture spiritual and social support important for quality of life. The study will help at intervention level by promoting family support, spirituality and support from the community.
The present study was aimed to find out distress in miscarrying women. Other aim was to expose the predictive relationship of religious rituals, spiritual support and social support with level of distress in women.
• There is likely to be a relationship between social support, spiritual support and religiosity and distress (depressive symptoms), in miscarrying women.
• Social support, spiritual support, religiosity and number of miscarriages will likely to predict distress in miscarrying women.
Correlational research design was used in the preset study.
In the present correlational study, purposive sampling was used. The participant was taken from two hospitals and one private clinic which granted permission for data collection. The sample comprised of 100 women (50 women who had miscarriage and 50 women of control group that would be matched on five variables i.e. age education, income, family system, occupation and women having no children
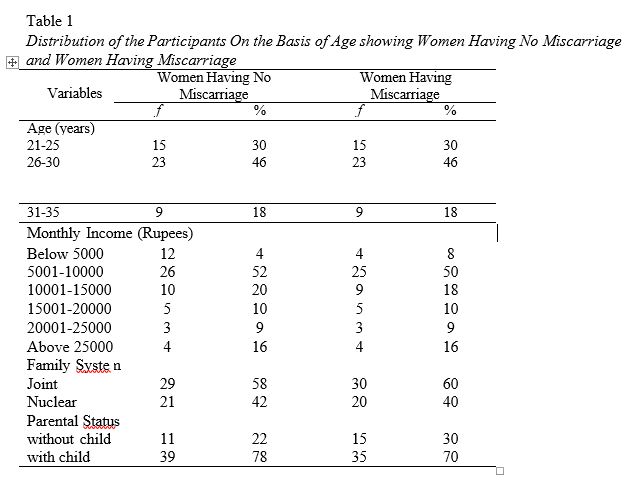
Table depicts that women having miscarriage and women having no miscarriage do not differ in their age. It also illustrates that there is no significant association between age and nature of groups.
Religious activity scale (RAS: Sitwat, 2005). This scale was developed by Sitwat (2005). It consists of questions regarding the performance of religious rituals such as prayers five times a day, fastening, reciting the Holy Quran, reading other Islamic literature etc. each item has rated according to level of personal effort and/ or frequency of rituals on 1- 5 scale. Its reliability reported for 12 items was 0.71.
Spiritual support scale (SSS: Maton, 1989). Maton developed scale in 1989. This scale consists of three items that are “I experience God‟s love and care on regular basis”, “I experience a close relationship with God and religious has been central to my coping”. Participants answered each item on five point scale. The scale was positively related to indice4s of religion and its value of Cronbach alpha was 0.95.
Multidimensional scale of perceived social support (MSPSS: Zimert et all., 1988). This scale is a validated measure of perceived social support. Social support is believed to contribute a moderating influence between stressful life events and depression. It consists of 12 items and is made to find thinking pattern about assistance from family, friends and other significant members of family and society. The items are broken down into factor groups in relation to origins of support with scores ranging from 1-7. Translated version was used in this study.
Center for epidemiologic studies depression scale (CES- D: Radloff, 1977). It consists of 20 items and it measures level of depressive symptoms in general population. Four of the items are positively worded to control for biases caused by response. Subjects are questioned to rate each item on scale of 0 to 3. In this 0 = rarely or none of time, 1= some or little of the time, 2= occasionally and moderate amount of time and 3= most or all of the time. The scores range from 0-
60. The reliability and validity of CES- D have been applied in African, Asian American, French and Greek countries and it was proved to be valid test. Translated form of CES-D was used in this study to find out level of distress among miscarrying as well as control group women.
Demographic questionnaire. Demographic variables are categories of variables that are measured in survey research design. In present research, demographic variables included were age, income, physical and mental health, number of pregnancies, number of miscarriages, duration after last miscarriage, current status that is pregnant or non-pregnant, number of children etc.
First of all permissions were taken from the authors of tool. After that, two of the tools were translated into Urdu. Translation was done by five individuals having 16 years of education. Then it was back translated and finalized by the help of supervisor and senior psychologist. Data were collected from one government hospital, one private hospital and two private clinics. All institutions granted permission for data collection. Women were selected through purposive sampling according to inclusion criteria after taking their consent. Matched group was taken from the community. Four questionnaires were used although there was no time limit for the test but approximately it took half an hour.
First of all departmental permission was taken to conduct the study. The authority letters were taken from the head of Center for Clinical psychology. The approval was also taken from the concerned person of psychiatric department by providing accurate information. Consent was taken from the participants of the study. The participants were briefed about the study. The results were accurately reported.
It was hypothesized that there will be relationship between social support, spiritual support, religiosity and level of distress. Pearson product moment correlation analysis was used to test hypothesis. The results of correlational analysis are presented I the table below:
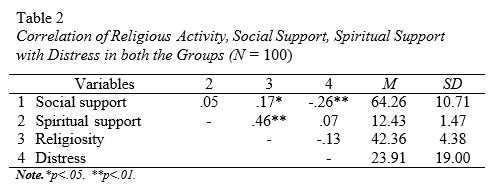
Table depicted that social support was negatively correlated with level of distress in both groups. However, the correlation in miscarriage women among social support and distress is significant. From the findings of the correlation analysis following predictors are emerged as social support and number of miscarriages thus regression analysis was run on these predictors.
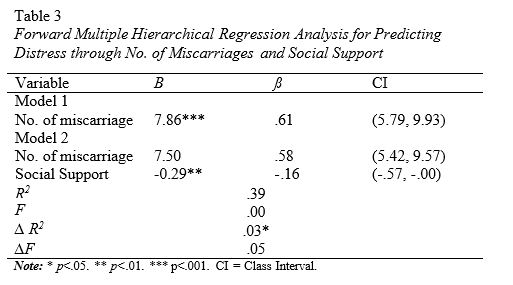
Table shows that no. of miscarriage significantly predicts level of distress and in model 2 no. of miscarriage and social support significantly predicts level of distress in women with miscarriage.
The present study examined the distress in miscarrying women. It also explored the relationship of religiosity, social support or spiritual support with the level of distress. It was hypothesized that there is likely to be a relationship between level of distress, social, spiritual support and religiosity in miscarrying women. It was proved that distress, social support, spiritual support, and religiosity are associated. This is consistent with previous literature, as many studies conducted in past have found that spirituality and religion may protect the consequences of stress and depression as well as help the diseased overcome attacks of pathology. The link between depression and spirituality has even found in cross generational gap studies. One study conducted with 60 mothers and 151 children, shown that daughter of women who think religion is important were 60 % less likely to have major depression at the 10 years follow up (Learnwell, 2009). As we are living in collectivistic culture, social support is very important for wellbeing. Similarly in this study majority of the participants were living in joint family system so this is the major buffering factor against distress. Present study also found that there is less distress in women having high religious practices. Results demonstrated that level of distress in women was showing slightly negative correlation with the level of religious practices, however results proved it insignificant. These results were consistent with the research of Conner and Conner (2002) which illustrated that religiosity was not associated with psychological distress. As a part of Muslim community religion plays an important role in psychological wellbeing. As most of the sample in the study was inclined towards religious practices so this is also an important factor in decreasing distress. It was also hypothesized that there would be less distress in women having high social support. Assumption was supported but at the same time it indicated negative correlation between distress and social support. These results were in accordance with the results of study conducted by Samuel, Hyancith, and Innocent (2008), which suggested that the presence of high social support is a protective buffer against depressive symptoms. The results of the study also depicted that social support and distress were negatively correlated. Social support is an important factor in coping distress. However, number of miscarriages seemed to be positively correlated with level of distress in miscarrying women. It was hypothesized that social support, spiritual support, religiosity and number of miscarriages will likely to predict distress in miscarrying women. The results of analyses showed that social support and number of miscarriage are significant predictors. This hypothesis was supported as social support appears to be the predictor of distress in miscarrying women. The results were in accordance with the previous study as Conway (1995) founds that psychological high pitched sound following miscarriage found to feeling sad and depressed. Previous research studies have shown that depressed people who have low social support remain depressed longer than those who have warm friends and family members (Moos & Cronkite, 1999). Number of miscarriage will predict distress in miscarrying women; this hypothesis was supported and is in accordance with the previous studies which report that miscarriage and induced abortion are life events that can potentially cause mental distress. Women who had experienced a miscarriage had more mental distress than women who had undergone an abortion (Bourn & Moum, 2005).
It was concluded from the study that Social support, spiritual and number of miscarriages are related to distress in miscarrying women. Number of miscarriages and social support emerged as significant predictors of distress in miscarrying women. Religious activities and spiritual support were not prominently related with the level of distress.
The sample size was limited as time span for data collection was one month that may lead to less generalized results. All questionnaires administered are self-repot measure so there can be a possible factor of biasness.
Further research can be carried out with comparatively increased sample. Different psychological aspects such as anxiety depression should be studied in miscarrying women in more detail by using different measuring tools. Findings can be utilized by clinical psychologist to focus on cognitive restructuring and family functioning of the women who faced trauma related to miscarriage.
Argyle, M., & Hallahmi, B. B. (1975). The social psychology of religion. London: Psychological Revivals. Retrieved from http://trove.nla.gov.au/ work/10922198
Bourn, A. N. & Moum, T. (2005). The course of mental health after miscarriage and induced abortion: a longitudinal, five-year follow-up study. Retrieved from http://bmcmedicine.biomed central.com/articles
Brown,I.(n.d). Aboriginal health and wellness. Retrieved from http://www.niichro.com/mental%20health/men_1.html
Bupa. (2009). Miscarriage. Retrieved from http://hcd2
.bupa.co.uk/fact_sheets/html/miscarriage.html
Bushak, 2009 May ATO incident a cause of expulsion Retrieved from: https://thetech.com/2009/09/08/ato-v129-n34
Chamberrlain, G.V. (1996). Obstetrics by Ten Teachers. (16th ed.).
Great Britain: The Bath Press, Avon
Cheng, S. T. & Chan, A. C. (2004). The multidimensional scale of perceived social support: dimensionality and age and gender differences in adolescents. Personality and Individual Differences, 37 (7), 1359-1369. Retrieved from http://www.sciencedirect.com /science
Chohan, A. (2005). Fundamentals of Gynecology (1st ed.) Retrieved from https://time traders/time publishers/timelasercom.
Conway, K. (1995). Miscarriage experience and the role of support systems: a pilot study. British Journal of Medical Psychology, 68(3), 259-267. Retrieved from http://www.ncbi.nlm.nih.gov
/pubmed/8527360
Conner, O., Cobb, J., & Conner, R.C. (2002). Religiosity, stress and psychological distress; no evidence for an association among indergraduates. Personality and Individual differences, 34(2), 2011- 2017.
Dasti, R. & Sitwat, A. (2005). Development of a Multidimensional Measure of Islamic Spirituality (MMIS). (Unpublished thesis).Center for Clinical Psychology, Punjab University, Lahore.
Elsunbruch, S. (2007). Social support during pregnancy: effects on maternal Depressive symptoms, smoking and pregnancy outcome. Human Reproduction, 22(3), 2869-2877. Retrieved fromhttp://humrep.oxfordjournals.Org/cgi/content /full/22/3/869
Fontana, D. (2003). Psychology, Religion, and Spirituality. UK: MPG Book, Ltd. Blackwell Publishing Ltd.
Glock, C. Y. & Stark, A. (1975). Adolescent Prejudice. New York: Harper