Depression, Anxiety, Coping and Quality of Life among Elderly Living in Old Age Homes and in Family Setup
*Nadab Parshad
Kinnaird College for Women, Lahore
Amjad Tufail, Ph.D.
Govt. M.A.O College, Lahore
The present study explored differences in depression, anxiety, coping and quality of life between elderly residing in old age homes and within family setup. It was predicted that elderly in old age homes will have higher depression, anxiety and poor quality of life however no difference on coping was predicted between the two groups. A sample of 120 elderly: 60 from old age homes and 60 from family setup participated. The measures used were: Pakistan Anxiety and Depression Questionnaire, Brief COPE Inventory and World Health Organization Quality of Life Questionnaire. Data was analyzed using Independent sample t-test. Results revealed high scores on depression, anxiety and quality of life among elderly residing in old age homes compared to elderly living with their families. Moreover, elderly living in old age home used more of maladaptive coping and elderly living with families used more of adaptive coping strategies.
Keywords: : Depression, Anxiety, Coping, Quality of Life, Elderly, Old Age Homes, Family Setup
The current study was undertaken to investigate differences on depression, anxiety, coping and quality of life between elderly living in old age homes and within family setup. Surprisingly, there is a dearth of literature on psychological issues faced by older people in Pakistan. As we are aware that a silent transformation has happened in the most recent 100 years and the greatest accomplishment of the century is longevity, globalizing and urbanization. As these changes are taking place, the meaning of old age is changing across families, cultures and countries (Bergeron, 2001).
Traditionally, Pakistani families have provided the older members of family with social security. On the other hand, it has been observed that in recent years there has been a noticeable change in the conventional Pakistani family system. Nowadays, families are moving from joint family system into nuclear system. Unfortunately, such changes in family systems, have transformed position of the elderly in the family and conventional family role is replaced by old age homes (Kramer et al., 2005). Thus, feelings of being isolated and poor social relationships along with decrease in physical and cognitive functioning makes older people more venerable to psychological problems (Cano et al., 2003; Marino, Sirey, Raue, & Alexopolous, 2008).
World Health Organization indicates that approximately 15% of elderly people aged 60 years and more often experience mental disorders (World Health Organization, 1999). Mental Health Foundation (2009) statistics indicates that 20% of elderly living in community and 40% living in old age homes suffer from depression (McEvoy, 2013). Moreover 10 to 20% of the elderly suffer from anxiety. Generally older population complains more about physical symptoms in depression rather than low mood as compared to young adults suffering from depression (Baldwin, 2002; Baldwin, 2008). Anxiety and feelings of irritability are often reported by elderly (Shulman, 1989). Moreover they report that they are unable to cope with such symptoms. Also, complaints of sleep and appetite disturbance, loss of energy and lack of interest in activities are common between elderly with depression. Often older people also experience co-morbidity of depression and anxiety disorders. Personality traits of a person, such as coping skills, are important resources in late life, since they prevent the onset of psychological problems (Beekman et al., 2000).
Coping is a progressive, dynamic and life-protecting process for adjusting to continuous changes of life. According to Lazarus and Folkman (1984) coping can be described as ones efforts to deliberately reduce or manage their psychological or social demands that are considered as difficult or demanding. When individuals are faced by a traumatic event, they use various strategies to cope with stressful situation. Thus, coping is classified on the bases of individual perspective and its utilization depends on health and nature of the elderly. Elderly are constantly faced by a number of challenges due to ageing process, loss of loved ones, chronic illnesses, and physical disabilities. Therefore older people utilize three most important coping styles while trying to decrease or eliminate a stressor: problem focused coping, emotional focused coping and avoidant coping. An adaptive form of coping is known as problem focused coping whereas emotional focused coping and avoidant coping is maladaptive coping. Being flexible and enhancing coping skills can help elderly to adjust to social, physical and psychological changes in old age (Warnick, 1995). Once elderly will learn to cope with changes of life, they have less mental health problems and better quality of life (Warnick, 1995).
Quality of life is an extensive concept, dynamic and continuous process, which changes over time and with life events. WHO (1999) describes quality of life as the perception one holds about their position in life, their apprehensions, standards and expectation of goals are all in accordance to the cultural values and norms in which they reside. It encompasses ones physiological and psychological well being, social relationships, and degree of freedom etc. Psychological approach to quality of life is related to an individual’s life satisfaction and well-being. Generally, quality of life for older people is beyond their physiological or psychological health, emotional well being and social relationships. There is a significant association between number of years of life and quality of life which can be decreased because of mental health problems. Therefore, coping intermediates with depression, anxiety, and quality of life; while an individual’s psychological health depends on his/her quality of life.
Good mental health, adaptive coping and higher quality of life are essential for promoting good health among elderly. Therefore the current study attempts to find difference on depression, anxiety, coping and quality of life between elderly living in old age homes and within family setup. The objective is to explore the psychological problems of elderly living in the community. This study will help to assess coping mechanisms and quality of life of elderly people living in different life situations and the impact of such situations on their lives.
Hypotheses
- Elderly living in old age homes and in family setup are likely to differ on depression.
- Elderly living in old age homes and in family setup are likely to differon anxiety.
- Elderly living in old age homes and in family setup are likely to on differ coping.
- Elderly living in old age homes and in family setup are likely to differon quality of life.
Method
Sample
Total sample consisted of 120 elderly, of which 60 elderly were from old age homes and 60 elderly were from family set-up were selected through purposive sampling. About 52% of elderly were aged 60-70 years whereas 47% elderly were aged 70-80 years (M=1.48, SD= .501). Equal number of males 50% and females 50% were included in the study. About 60% of the elderly were widow/widower, 30% were married, 6% were unmarried and 2% were divorce or separated. Almost 40% of elderly were receiving pension, 41% were earning through other sources (i.e. business, rent etc.) and 18% were still doing jobs. Most of the elderly (79%) were living in nuclear family system as compared to 20% residing in joint family system.
Assessment Measures
Pakistan Anxiety and Depression Questionnaire (PADQ). Pakistan Anxiety and Depression questionnaire (Mumford et al., 2005) measures anxiety and depression in Pakistani population. It is a self- report questionnaire which contains 30 items. It includes two subscales; 15 items of anxiety and depression each. All items are to be answered as yes=1 and no=0 scores. A total score of 6 or more on anxiety or depression subscale indicates probable anxiety or depression disorder. Pakistan Anxiety and Depression Questionnaire has reliability with Cronbach alpha ranging from .90 to .94 for anxiety subscale and .91 for depression subscale.
Brief COPE Inventory (COPE). The Brief COPE Inventory (Carver, 1997) measures individual styles of coping. In this study an Urdu translated version (Jibeen & Khalid, 2010) was used. It is a self- report questionnaire containing 28 items, with a four point Likert scale. The Brief COPE determines 14 dimensions. The author has not suggested any particular instructions for scoring but generating dominant coping styles. For the translated version the Cronbach alpha for problem-focused coping is .74 and for emotion-focused coping is .63.
World Health Organization Quality of Life Questionnaire (WHO QOL-BREF). WHO Quality of Life Questionnaire (WHO, 1998) is developed by World Health Organization to measure quality of life, which consists of 26 items. In this study an Urdu translated version by World Health Organization was used. It measures four dimensions; physical domain, psychological domain, social relationships and environmental domain. Higher scores signify higher quality of life among individuals. The questionnaire shows discriminant validity, content validity and test-retest reliability.
Procedure
The sample was recruited from a public and a private old age home in Lahore. Elderly living with their families were recruited from urban areas of Lahore; Model town, Johar town, Iqbal town and Faisal town. Permissions were sought from the authors of the instruments and the authorities of selected old age homes. After getting permission from authorities, a formal consent form was taken from the participants of both settings. The participant’s were briefed about the aim and the instructions regarding questionnaires were explained to them. Group administrations of the questionnaires were carried out. However participants with chronic illnesses (heart patients, cancer etc) and with severe visual and hearing disability were not included in the study. In case of any difficulty in following instructions or understanding the statements, participants were provided with assistance. There was no limitation of time for elderly.
Results
Independent sample t-test was used to compare elderly living in old age homes and within family setup on depression, anxiety, coping and quality of life.
Table 1 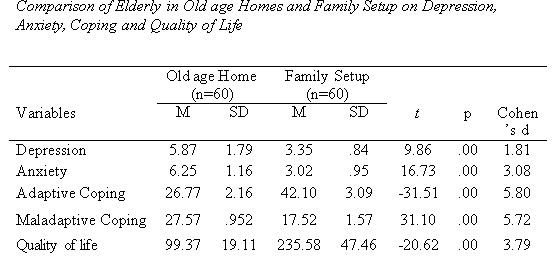
Table 1 shows significant differences in both groups and all proposed hypothesis are proved. Elderly living in old age homes reported more symptoms of depression and anxiety use maladaptive coping strategies and have poor quality of life in comparison to elderly living in family setup.
Discussion
Present study aimed to explore differences on depression, anxiety, coping and quality of life between elderly living in old age homes and in family setup. The findings revealed significant differences on depression, anxiety and quality of life between elderly residing in old age homes and in family setup. Comparison on depression, anxiety and quality of life revealed that there were more problems faced by elderly who were residing in old age homes compared to the one’s residing with their families. The findings were in agreement with the study conducted by Agarwal and Srivastava (2002) which suggested that psychological problems like depression, anxiety, loneliness, neglect by family members, social isolation were more common between elderly living in old age homes. The findings were also supported from the study by Guha and Valdiya (2000) which suggested that psychiatric morbidity of elderly in old age homes was 266.7% and for those living in community was 10%. Similarly, Rahman (2013) examined prevalence of anxiety (58.3%) and depression (81%) was high among elderly in old age homes compared to anxiety (36.6%) and depression (56.1%) among elderly living in their homes.
In Pakistani society, the status of older people living with their families is greater. In most families the wisdom and experience of older people is respected and honored. Thus, elderly living with their families experience less depression and therefore higher quality of life than elderly living in old age homes Most elderly residing in old age homes are widow/widower, have low or no income and also lose their influence, their active roles in family and society also decrease (Chohan, 2007). They therefore lose their ability to carry out activities of daily life due to which they are faced by worries about ability to look after themselves in future. Moreover most of the elderly in old age homes suffer from negative life events like divorce, loss of spouse, rejection of care and support by family members, which makes them more prone to psychological problems than elderly living with their families (Rahman, 2013). Physical health problems are also more common among elderly in old age homes (Rao, Chennamsetty, & Kuna, 2014). Naik (2007) reported significant differences on quality of life with elderly living with their families having better quality of life than those living in old age homes. These findings were also supported by other studies (Kavitha, 2007; Mathew, George, & Paniyadi, 2009; Yadidya, 2003). Furthermore, there is lack of privacy, restricted environment, low emotional support, low social activity, and lack of care facilities in old age homes due to which they have poor quality of life. Older people living in old age homes feel negative emotions like; loneliness, social isolation, disabilities and also suffer from prolong illnesses. All such factors either independently or combined undermine self-respect and self-esteem of elderly and that leads to a growing sense of sadness, anxiety and poor quality of life (Chohan, 2007).
Also, findings revealed a significant difference on coping between elderly living in old age homes and in family setup. It was found in present study that elderly who were residing in old age homes used more of maladaptive coping strategies while elderly residing with their families used more of adaptive coping strategies to cope with different situations. The findings were consistent with previous studies which suggested that elderly living in old age homes use more of maladaptive coping strategies (behavioral disengagement, denial, self-distraction, self-blame, substance use and venting) rather than using adaptive coping strategies (active coping, instrumental support, planning, acceptance, emotional support, humor, positive reframing and religion) (Beena, 2006; Rohini, 2011). Moreover, coping strategies are significantly associated with psychological problems in late life (Beena, 2006). Elderly with psychological problems use more of maladaptive coping strategies (Rohini, 2011). To cope with stressors elderly living in old age homes make more use of religious beliefs and faith. Religious beliefs can help elderly to achieve better mental health and faith in God can provide them strength to fight with psychological problems. Hence, frequent use of maladaptive coping; emotion focused coping and use of less social support as coping method makes it difficult for elderly in old age homes to cope with mental health problems (Beena, 2006).
Conclusion
Old age had never been a problem for Pakistan because the traditional joint family system has provided the elderly with respect, support and social security. However, from past few years there has been a distinct change in the traditional Pakistani family system. Joint family system is now revolving into nuclear family system. With the change in family systems, the status of elderly have reformed and now the traditional family role is being shared by institutions like old age homes. Feelings of low social support and loneliness along with age related decline in cognitive and physical functioning make the elderly prone to psychological disturbances.
Thus the psychological problems are more prevalent among elderly residing in old age homes. Moreover, the psychological problems contribute to maladaptive coping and low quality of life among elderly living in old age homes. On the other hand, elderly living with their families are mostly provided with respect, emotional and social support thus contributing to less psychological problems. Elderly with less psychological problems use more adaptive coping strategies, and therefore have better quality of life. Nevertheless, these issues address the need for preserving our traditional values of joint family system and we need to focus on the mutual support and understanding between the older and younger generation, so that the older generation can lead a respectful and meaningful life.
Limitations and Recommendations
- There is limitation of sample size (n=120) thus it should be increased for future studies.
- Further investigation should include more old age homes as only two old age homes were selected in the present study.
- Data was collected from Lahore city only, other cities of Pakistan should be incorporated for future research.
- Data was collected using purposive sampling technique; therefore the results of the present study cannot be generalized to larger sample.
- Moreover little research has been done on elderly especially those living in old age homes, therefore more research should be conducted on elderly and the issues faced by them.
Implications
Older people are a special concern group and therefore they need special consideration. There is a need to develop programs to increase social interaction of elderly with others (e.g. group activities). Government and heath care services should provide more physical and mental health care and facilities for elderly living in old age homes. There is scope to reduce mental health problems, enhance adaptive coping skills, and improve quality of elderly. Therefore, heath care services and counseling programs should be organized for elderly staying at home or living in old age homes.
References
Agarwal, S., & Srivastava, S. K. (2002). Effect of living arrangement and gender differences on emotional states and self-esteem of old aged persons. Indian Journal of Gerontology, 16, 312- 320.
Baldwin, R., Chiu, E., Katona, C., & Graham, N. (2002). Guidelines on depression in older people: Practising the evidence. London: Martin Dunitz Ltd.
Baldwin, R. (2008). Mood disorders: Depressive disorders. In R. Jacoby, C. Oppenheimer, T. Dening & A. Thomas (Eds.), Oxford Textbook of Old Age Psychiatry. Oxford: Oxford University Press.
Beekman, A. T., de Beurs, E., van Balkom, A. J., Deeg, D. J., van Dyck, R., & van Tilburg, W. (2000). Anxiety and Depression in Later Life: Co-Occurrence and Communality of Risk Factors. American Journal of Psychiatry, 157(1), 89-95.
Beena, T. (2006). Assess the psychological problems and coping strategies of elderly women residing in an selected old age at Mangalore. Unpublished thesis. Dr. M.V. Shetty Institute of Health Sciences, Mangalore, India.
Bergeron L. R. (2001). An elderly abuse case study: Case gives stress or domestic violence. Journal of Gerontogical Social Work, 34(3), 47-63.
Cano, A., Scaturo, D. J., Sprafkin, R. P., Lantinga, L.J., Fiese, B.H., & Brand, F. (2003). Family support, self-rated health and psychological distress: Primary care companion. Journal of Clinical Psychiatry, (5), 111-117.
Carver, C. S. (1997). You want to measure coping but your protocol's too long: Consider the Brief COPE. International Journal of Behavioral Medicine, 4, 92-100. doi:10.1207/s15327558ijbm0401_6
Chohan, A. R. (2007). Social isolation in old age, responsibilities of family members, rights of senior citizens, a case study of Quetta district. Unpublished thesis. University of Balochistan, Quetta, Pakistan.
Guha, S., & Valdiya, P. S. (2000). Psychiatric morbidity amongst the inmates of old age home. Indian Journal of Psychiatry, 42 (44).
Jibeen, T., & Khalid, R. (2010). Predictors of psychological wellbeing of Pakistani immigrants in Toronto, Canada. International Journal of Intercultural Relations, 34, 452-464.
Kramer, S. E., Hella, G., Allessie, M., Dondorp, A. W., Zekveld, A. A., Kapteyn, T. S. (2005) A home education program for older adults with hearing impairment and their signfificant others: a randomized trial evaluating short- and long-term effects. International Journal of Audiology, 44, 225–264.